SONOGRAM ABBREVIATIONS
Ao Aorta
Bl Bladder
K Kidney
L Liver
Sp Spleen
KEY WORDS
Angiomyolipoma ( AML ). Unusual (1%), benign, fatty tumor of the kidney that is usually seen in middle-aged women. AML also occurs in approximately 80% of patients with tuberous sclerosis.
Calyceal Diverticulum. Postinflammatory fluid-filled structure adjacent to a pyramid.
Calyx. A portion of the renal collecting system adjacent to the renal pyramid in which urine collects and that is connected to an infundibulum.
Column of Bertin. Sometimes the calyces and the infundibulum bud from the pelvis in two groups. The intervening normal parenchyma can falsely raise suspicion of a tumor and is known as a column of Bertin.
Dromedary Hump. A bulge off the lateral margin of the left kidney—a normal variant.
Fibrolipomatosis. Excess fat deposition in the center of the kidney; seen with aging.
Hydronephrosis. Dilatation of the pelvic collecting system due to obstruction.
Infundibulum. Funnel-shaped tube connecting the calyx to the renal pelvis. Also known as a major calyx.
Intravenous Pyelogram (IVP, IVU, EU). Classic method for imaging the genitourinary tract. A conventional x-ray examination of the kidneys, ureters, and urinary bladder after the injection of a radio-opaque contrast agent (“dye”). Rapidly being supplanted by computed tomography.
Nephroblastomatosis. An abnormal persistence of normal embryonic tissue into infancy and childhood. This persistent tissue can be diffuse, multifocal, or unifocal, and can behave along a spectrum from normal variant to malignant tissue (Wilms’ tumor). Nephroblastoma is a synonym for Wilms’ tumor.
Polycystic Kidney Disease. A relatively common hereditary disease in which multiple cysts develop on each kidney. There are two forms relating to the mode of heredity and time of onset.
Pseudotumor. Overgrowth of a portion of the cortex indenting the sinus echoes and simulating a tumor.
Renal Cell Carcinoma (RCC) (also known in the past as hypernephroma or Grawitz Tumor). Adenocarcinoma of the kidney that accounts for almost 90% of all primary malignant renal parenchymal tumors.
Renal Pelvis. Centrally located sac into which the various infundibula drain. The pelvis drains into the ureter.
Transitional Cell Carcinoma (TCC). A tumor of the kidney, collecting system, ureter, or bladder lining cells that often recurs in another site in the genitourinary tract after removal. TCC accounts for approximately 7% of all primary malignant renal parenchymal tumors.
Tuberous Sclerosis (TS). A disease whose triad is characterized by skin lesions, epileptic seizures, and mental deficiency. AMLs associated with TS are classically small, multiple, and bilateral. TS is also associated with renal cysts, and uncommonly, renal cell carcinoma (RCC).
Uric Acid Calculus. A renal stone that is invisible on plain radiographs.
von Hippel-Lindau (VHL) Disease. A hereditary syndrome that has a greatly increased risk for a variety of cancers, including RCC in approximately 40%.
Wilms’ Tumor. Most common malignant renal lesion seen in children.
The Clinical Problem
Although the intravenous pyelogram (IVP) was a common method of detecting renal masses in the past, it does not effectively aid in deciding whether such a mass is fluid filled (a cyst) or solid tissue—a decision that can generally be made easily with ultrasound. Cysts are managed by benign neglect (or rarely cyst puncture), whereas tumors require surgical resection or ablation (radiofrequency or cryoablation).
In the United States, computed tomography (CT) is often used in the further investigation of renal masses, but the nature of some renal masses may be confusing on CT and may be clarified by ultrasound and Doppler. Clinical symptoms related to the kidney may include pain, fever, urinary frequency and urgency, a palpable mass, hematuria, pyuria, white cells, and protein in the urine. With the increased frequency of imaging today, tumors may be clinically silent and discovered incidentally when the study is being performed for other reasons.
Anatomy
See Chapter 17.
Technique
See Chapter 17.
Do not perform a sonogram without first examining the report and images of the IVP or CT scan (if available), so you know what you are looking for. Doppler is helpful for examining the inferior vena cava and renal vein to detect tumor involvement. Be alert for stones, their posterior acoustic shadowing, and the associated “twinkle artifact” on color Doppler (see Chapter 20). With the use of these techniques, stones sometimes are readily visible on ultrasound when hard to see on plain films.
Pathology
FLUID-FILLED MASSES
Renal Cysts
Renal cysts are rare in children, gradually becoming more frequent with age. In the elderly, they are very common. They may be single (Fig. 18-1) or multiple (Fig. 18-3). The sonographic features of a cyst are as follows:
1. Acoustic enhancement (good through transmission with a strong back wall) (Fig. 18-1)
2. Usually a smooth spherical outline with thin walls
3. Usually fluid filled with no internal echoes
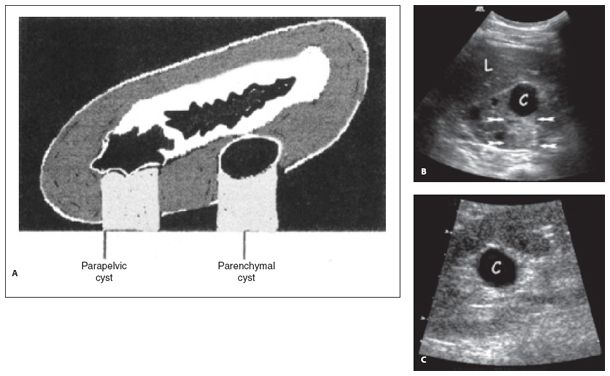
Figure 18-1. ![]() A. Diagram: Parenchymal cyst at the midpole of the kidney shows good through transmission, smooth borders, and absence of internal echoes. Parapelvic cyst at the upper pole has an irregular outline. Parapelvic cysts can be mistaken for dilated calyces. B. Sonogram: cortical parenchymal cyst (C). Note enhanced through transmission behind it (arrows). Other smaller cysts elsewhere in this kidney are also noted. C. Sonogram: Parapelvic cyst (C) in a different patient shows a well-defined anechoic mass centered in and distorting the renal sinus fat.
A. Diagram: Parenchymal cyst at the midpole of the kidney shows good through transmission, smooth borders, and absence of internal echoes. Parapelvic cyst at the upper pole has an irregular outline. Parapelvic cysts can be mistaken for dilated calyces. B. Sonogram: cortical parenchymal cyst (C). Note enhanced through transmission behind it (arrows). Other smaller cysts elsewhere in this kidney are also noted. C. Sonogram: Parapelvic cyst (C) in a different patient shows a well-defined anechoic mass centered in and distorting the renal sinus fat.
Unusual cysts may have irregular walls and may contain low-level echoes in a dependent position owing to debris. Debris may be confused with spurious echoes related to the slice thickness artifact (Fig. 18-2; see also Chapter 57).
Septa dividing a cyst into compartments may be seen (Fig. 18-2). Such septa prove that a cyst is fluid filled but may be difficult to visualize completely and may be mistaken for a mural mass.
Irregular borders, septations, or debris should raise the question of malignancy or necrosis and require further investigation, usually by CT.
Peripelvic cysts may be centrally located and hard to distinguish from a dilated pelvis or calyx (Fig. 18-1). Their shape is often irregular.
The Bosniak classification of renal cysts is a grading system originally developed for CT but is now commonly used in magnetic resonance imaging. It uses morphologic criteria to divide cystic masses along a spectrum from benign (Category I) to obviously malignant (Category IV), allowing one to decide whether a lesion can be ignored, requires follow-up, or requires surgery. However, because the system relies on the assessment of both calcifications and soft-tissue enhancement within the mass, its usefulness has not been rigorously evaluated when cystic masses are imaged by ultrasound. Perhaps when ultrasound contrast agents are widely available in the United States, this system will be reevaluated; regardless, it is useful to be familiar with the general Bosniak concept because radiologists and urologists commonly use the terminology.
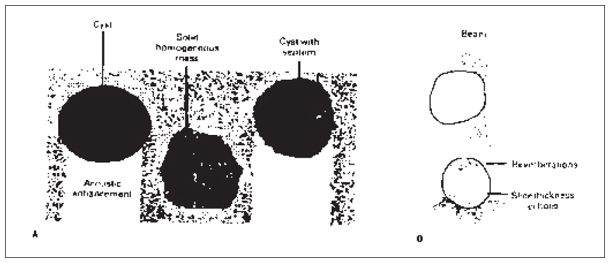
Figure 18-2. ![]() Cyst versus solid homogeneous mass. A. Diagram showing the difference between a cyst and a solid homogeneous mass. Through transmission beyond a solid homogeneous mass is limited, although there will be a back wall, and there are usually a few internal echoes. Septa within a cyst are incompletely seen unless they are at right angles to the acoustic beam. B. Artifactual echoes caused by reverberations and slice thickness effect. (For details of how these artifacts develop, see Chapter 57.)
Cyst versus solid homogeneous mass. A. Diagram showing the difference between a cyst and a solid homogeneous mass. Through transmission beyond a solid homogeneous mass is limited, although there will be a back wall, and there are usually a few internal echoes. Septa within a cyst are incompletely seen unless they are at right angles to the acoustic beam. B. Artifactual echoes caused by reverberations and slice thickness effect. (For details of how these artifacts develop, see Chapter 57.)
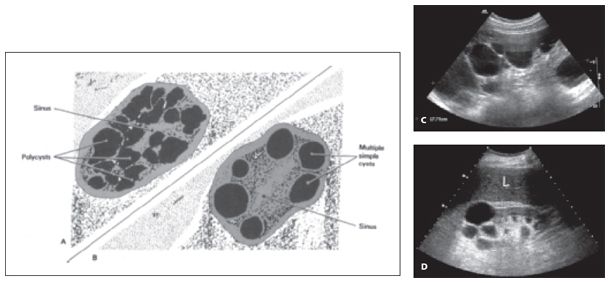
Figure 18-3. ![]() Multiple cysts. A. Cysts in polycystic disease have irregular walls and are variable in size. They distort the renal sinus echoes. B. Multiple simple cysts have smooth walls, are not nearly as numerous, and vary less in size. C. Classic sonogram for hereditary autosomal dominant polycystic kidney disease. Note multiple cysts and large size (~18 cm). The opposite kidney appeared the same. D. Multiple simple cysts in a different patient.
Multiple cysts. A. Cysts in polycystic disease have irregular walls and are variable in size. They distort the renal sinus echoes. B. Multiple simple cysts have smooth walls, are not nearly as numerous, and vary less in size. C. Classic sonogram for hereditary autosomal dominant polycystic kidney disease. Note multiple cysts and large size (~18 cm). The opposite kidney appeared the same. D. Multiple simple cysts in a different patient.
Adult Polycystic Disease
Renal cysts in patients with polycystic disease usually have an irregular outline and are of markedly varied size (Fig. 18-3
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


