Abstract
Neural tumors are the most common primary tumors in the posterior mediastinum, but metastases, lymphoma, and primary bone tumors do occur in this location. Vertebral fractures often have associated hematomas, and discitis with osteomyelitis may extend into the paravertebral soft tissues. Aortic aneurysm, dissection, or injury may all cause hemorrhage with hematoma in the posterior mediastinum. Bochdalek hernias are in the posterior inferior mediastinum and may contain a kidney. Neurenteric cysts have associated vertebral anomalies and are more posterior than the other congenital cysts. Extramedullary hematopoiesis is rare but should be suspected in patients with chronic anemias.
Keywords
aortic aneurysm, aortic dissection, Bochdalek hernia, extramedullary hematopoiesis, ganglioneuroblastoma, gannglioneuroma, lateral meningocele, neural tumors, neurenteric cysts, neuroblastoma, neurofibroma, paraspinal abscess, schwannoma
Questions
- 1.
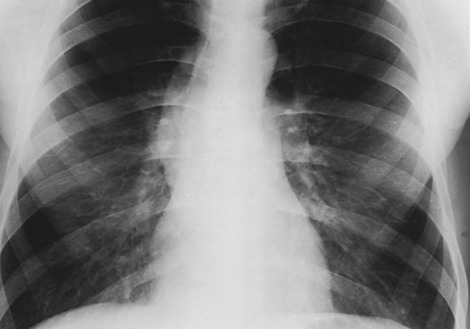
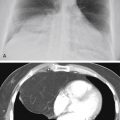
Which one of the following diagnoses is most likely for the case illustrated in Fig. 12.1, A-C ?
- a.
Neuroblastoma.
- b.
Paraspinal abscess.
- c.
Schwannoma.
- d.
Paraganglioma.
- e.
Neurenteric cyst.
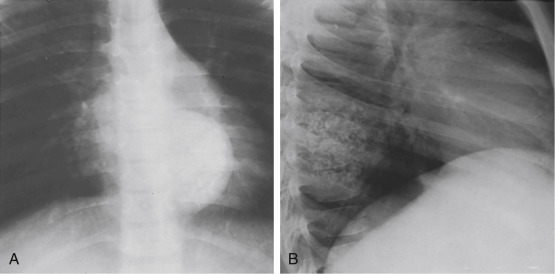
Fig. 12.2
- a.
- 2.
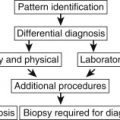
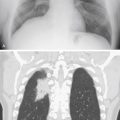
Which one of the following neural tumors is most likely in a 6-year-old patient ( Fig. 12.2, A and B )?
- a.
Ganglioneuroma.
- b.
Neurofibroma.
- c.
Ganglioneuroblastoma.
- d.
Schwannoma.
- e.
Chemodectoma.
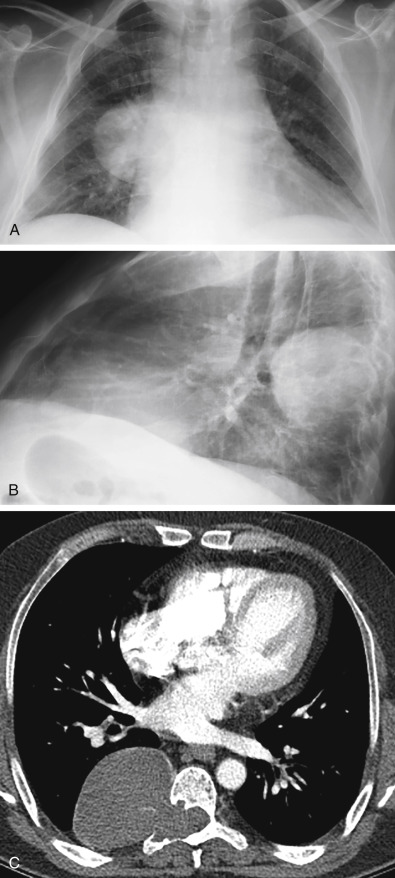
Fig. 12.1
- a.
- 3.
Which one of the following is most likely a vertical elongated mass with rib spreading and erosion of multiple ribs?
- a.
Neurofibroma.
- b.
Schwannoma.
- c.
Hemangioma.
- d.
Neuroblastoma.
- e.
Chemodectoma.
- a.
Match the following descriptions with the list of diagnoses that might cause a posterior mediastinal mass:
|
|
|
|
|
|
Discussion
This discussion follows the divisions of the mediastinum described by Felson. 150 The middle and posterior compartments of the mediastinum are divided by a line that follows the curvature of the spine and is located 1 cm posterior to the anterior border of the vertebral bodies. Therefore, most of the masses that are considered herein might be classified by other authors as posterior gutter masses. Very large masses often extend into the anatomic posterior mediastinum. It may be difficult to determine the origin of a very large mass and therefore to appreciate that it did arise in the posterior gutter.
Neural Tumors
The neural tumors constitute the largest group of posterior mediastinal and posterior gutter masses ( Chart 12.1 ) 61 and are derived from nerve roots, intercostal nerves, or sympathetic ganglia. Nerve root tumors are schwannomas or neurofibromas. The sympathetic ganglion tumors include the neuroblastomas, ganglioneuroblastomas, and ganglioneuromas. Paragangliomas, including chemodectoma and pheochromocytoma, are infrequent causes of posterior mediastinal masses. 459
- I.
Neoplasms
- A.
Neural tumors459
- 1.
Ganglion series tumors (e.g., neuroblastoma, ganglioneuroblastoma, ganglioneuroma)
- 2.
Nerve root tumors (e.g., schwannoma, neurofibroma, malignant nerve sheath tumor)
- 3.
Paragangliomas (e.g., chemodectoma, pheochromocytoma)
- 1.
- B.
Metastases
- C.
Lymphoma
- D.
Mesenchymal tumors (e.g., fibroma, lipoma, muscle tumors, leiomyoma)
- E.
Hemangiomas
- F.
Thyroid tumors
- G.
Vertebral tumors (e.g., osteoblastoma, giant cell tumor, multiple myeloma)
- H.
Solitarily fibrous tumor of the pleura 116
- A.
- II.
Germ cell tumors, including seminoma (rare in the posterior mediastinum) 453
- III.
Inflammation
- A.
Paraspinal abscess (e.g., tuberculosis, staphylococcus)
- B.
- C.
Lymphoid hyperplasia
- D.
Sarcoidosis
- A.
- IV.
Vascular lesions
- V.
Trauma
- A.
Traumatic pseudoaneurysm
- B.
- C.
Loculated hemothorax
- D.
Traumatic pseudomeningocele
- A.
- VI.
Developmental lesions
- VII.
Abdominal diseases
- A.
Bochdalek hernia (thoracic kidney) 351
- B.
Pancreatic pseudocyst or abscess 302
- C.
Retroperitoneal masses (e.g., germ cell tumors, sarcomas, metastases)
- A.
- VIII.
Other
- A.
Loculated pleural effusion (e.g., empyema)
- B.
Lateral meningocele
- C.
Lipoma and lipomatosis 251
- D.
Extramedullary hematopoiesis 282
- A.
Schwannomas are derived from the sheath of Schwann, which forms the connective tissues of the nerve root. There are no nerve cells in a schwannoma. This is in contrast to the true neurofibroma, which contains both Schwann cells and nerve cells. Before 1955, distinction between these two tumors was not generally made. This suggested that neurofibromas are the most common cause of posterior mediastinal masses. The schwannomas are much more common than true neurofibromas and are the most common of all the neural tumors. Most schwannomas and neurofibromas are benign tumors. The very rare malignant nerve root tumors were previously classified as a malignant schwannoma, regardless of the presence of nerve cells in the tumor, but have been reclassified as malignant nerve sheath tumors.
Neuroblastomas are highly malignant, undifferentiated, small round cell tumors that originate from the sympathetic ganglia. In contrast, the ganglioneuromas, which are also derived from the sympathetic ganglia, are completely benign. 123 Mature connective tissues, which resemble the connective tissues of schwannomas, are the primary tissues in ganglioneuromas. The presence of mature ganglion cells is the histologic feature that distinguishes schwannomas from ganglioneuromas. Ganglioneuroblastomas are mixed cell tumors that not only contain mature, well-differentiated ganglion cells, but also connective tissues and undifferentiated round cells. In other words, ganglioneuroblastomas have features of both ganglioneuromas, which are completely benign, and neuroblastomas, which are highly malignant. These tumors have a better prognosis than the neuroblastomas, but must be regarded as malignant tumors. It is true, however, that cases of spontaneous maturation have been observed. Cushing and Wolbach 105 have described a case that matured from a neuroblastoma to a completely differentiated ganglioneuroma; unfortunately, this is a very rare event.
The radiologic presentation of most neural tumors is a homogeneous opaque mass in the posterior mediastinum. A small percentage of these tumors contain calcification. 127 , 459 Calcification should be evenly distributed through a mass when the lesion is viewed in both the posteroanterior (PA) and lateral projections. The calcification often assumes a speckled pattern and may vary considerably in quantity ( Fig. 12.2, A and B ).
There is a striking difference between the shape of nerve root tumors and tumors of the ganglion series. 61 , 459 , 586 Of nerve root tumors, 80% appear as round masses (see Fig. 12.1, A-C ), whereas 80% of ganglion series tumors appear as vertically oriented, elongated masses ( Fig. 12.3 ). An additional feature that is helpful in distinguishing these masses is a tapered border, which suggests a ganglion series tumor. In contrast, round nerve root tumors tend to have a sulcus, which may indicate a more lateral position. This may suggest that the tumor is arising from the intercostal nerve. In Chapter 2 , schwannoma was mentioned as a possible cause of a chest wall mass. (Answer to question 1 is c .)