Posterior Tarsal Tunnel Syndrome and Other Abnormalities of the Posterior Tibial Nerve
Anatomic Considerations
The tibial nerve is one of the two major continuations of the sciatic nerve, the other being the common peroneal nerve (Fig. 10.1). The tibial nerve provides sensory innervation to the posterior portion of the calf, the heel, and the medial plantar surface. The tibial nerve splits from the sciatic nerve at the superior margin of the popliteal fossa and descends in a slightly medial course through the popliteal fossa. The tibial nerve at the ankle lies just beneath the popliteal fascia and is readily accessible for neural blockade. The tibial nerve continues its downward course, running between the two heads of the gastrocnemius muscle, passing deep into the soleus muscle (Fig. 10.2). The nerve courses medially between the Achilles tendon and the medial malleolus, where it divides into the medial and lateral plantar nerves, providing sensory innervation to the heel and medial plantar surface (Figs. 10.3 and 10.4). The tibial nerve is subject to compression at this point as the nerve passes through the posterior tarsal tunnel (Fig. 10.5). The posterior tarsal tunnel is made up of the flexor retinaculum, the bones of the ankle, and the lacunar ligament. In addition to the posterior tibial nerve, the tunnel contains the posterior tibial artery and vein as well as a number of flexor musculotendinous units.
Clinical Correlates
An uncommon cause of plantar foot pain, posterior tarsal tunnel syndrome, is caused by entrapment and compression of the posterior tibial nerve as it passes through the posterior tarsal tunnel (Fig. 10.5). The most common cause of compression of the posterior tibial nerve within the posterior tarsal tunnel location is trauma to the ankle, including fracture, dislocation, and crush injuries (Fig. 10.6). The boundaries of the posterior tarsal tunnel are the flexor retinaculum, the bones of the ankle, and the lacunate ligament. The posterior tarsal tunnel contains the posterior tibial nerve, vein and artery, tibialis posterior, flexor digitorum longus, and flexor hallucis longus musculotendinous units. These musculotendinous units are subject to the development of tenosynovitis, while the posterior tibial artery is subject to the development of aneurysms and posterior tibial vein is subject to the development of thrombophlebitis and varicosities (Fig. 10.7). Patients with rheumatoid arthritis have a higher incidence of posterior tarsal tunnel syndrome than the general population. Posterior tarsal tunnel syndrome is much more common than anterior tarsal tunnel syndrome.
Posterior tarsal tunnel syndrome presents clinically in a manner very analogous to carpal tunnel syndrome. Night-time foot pain analogous to the nocturnal pain of carpal tunnel syndrome is often present. The patient suffering from posterior tarsal tunnel will frequently complain of pain, numbness, and dysesthesias involving the plantar surface of the foot and may radiate into the medial ankle. The medial and lateral plantar divisions of the posterior tibial nerve provide motor innervation to the intrinsic muscles of the foot. The patient may note weakness of the toe flexors and instability of the foot caused by weakness of the lumbrical muscles.
Physical findings include tenderness over the posterior tibial nerve at the medial malleolus. A positive Tinel sign usually is present just below and behind the medial malleolus over the posterior tibial nerve (Fig. 10.8). Active inversion of the ankle often reproduces the symptoms of the posterior tarsal tunnel syndrome. Weakness of the flexor digitorum brevis and the lumbrical muscles may be present if the medial and lateral branches of the posterior tibial nerve are compromised.
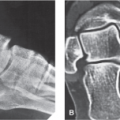
Posterior tarsal tunnel syndrome is frequently misdiagnosed as lumbar radiculopathy or diabetic neuropathy or is attributed to primary ankle pathology leading to both diagnostic and therapeutic misadventures. Plain radiographs of the ankle will help identify primary ankle pathology and electromyography will help distinguish the compromise of posterior tibial nerve associated with posterior tarsal tunnel syndrome from radiculopathy (Fig. 10.9). Most patients who suffer from lumbar radiculopathy have back pain associated with reflex, motor, and sensory changes that are associated with back pain, whereas patients with posterior tarsal tunnel syndrome have no back pain and no reflex changes. Furthermore, the motor and sensory changes of posterior tarsal tunnel syndrome are limited to the distribution of the medial and lateral plantar divisions of
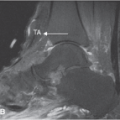
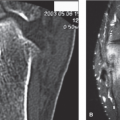
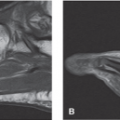
the posterior tibial nerve. Lumbar radiculopathy and posterior tibial nerve entrapment may coexist as the so-called “double crush” syndrome and this can further confuse the clinical picture. Based on the patient’s clinical presentation, additional testing may be indicated, including complete blood cell count, uric acid, sedimentation rate, and antinuclear antibody testing. MRI or CT scanning of the lumbar spine is indicated if a herniated disk, spinal stenosis, or a space-occupying lesion is suspected. MRI and/or ultrasound imaging of the posterior ankle and foot are indicated to confirm the diagnosis of posterior tarsal tunnel syndrome by identifying the pathology responsible for nerve entrapment, for example, tumor, mass, osteophyte, as well as to identify occult pathology (Figs. 10.10 to 10.14).
the posterior tibial nerve. Lumbar radiculopathy and posterior tibial nerve entrapment may coexist as the so-called “double crush” syndrome and this can further confuse the clinical picture. Based on the patient’s clinical presentation, additional testing may be indicated, including complete blood cell count, uric acid, sedimentation rate, and antinuclear antibody testing. MRI or CT scanning of the lumbar spine is indicated if a herniated disk, spinal stenosis, or a space-occupying lesion is suspected. MRI and/or ultrasound imaging of the posterior ankle and foot are indicated to confirm the diagnosis of posterior tarsal tunnel syndrome by identifying the pathology responsible for nerve entrapment, for example, tumor, mass, osteophyte, as well as to identify occult pathology (Figs. 10.10 to 10.14).
 FIGURE 10.1 The tibial nerve is one of the two major continuations of the sciatic nerve, the other being the common peroneal nerve. (From Tank PW, Gest TR. The lower limb. In: Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:119.) |
 FIGURE 10.2 The anatomy of the tibial nerve. (From Tank PW, Gest TR. The lower limb. In: Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:119.) |
 FIGURE 10.3 Relationship of the posterior tibial nerve and the tibial artery and vein.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|