Key Points
- ▪
Bioprostheses may develop transvalvar or perivalvar insufficiency, and mechanical prostheses may develop thrombotic or pannus-mediated obstruction or paravalvar insufficiency.
- ▪
The consequences of valve prosthesis dysfunction may be evident on the chest radiograph; left-sided prosthesis insufficiency or obstruction may result in radiographically evident heart failure.
- ▪
In the absence of another apparent reason, when a patient with a valvular prosthesis develops hemodynamic duress, the prosthesis should be suspected of dysfunction, until disproven.
Prosthesis Dysfunction
The presence of heart failure in a patient with a valve prosthesis warrants due consideration of prosthesis dysfunction.
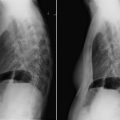
Bioprostheses are susceptible to transvalvar insufficiency due to wear-and-tear degeneration or infection and to perivalvar insufficiency, which is usually caused by infection ( Fig 12-1 ). Bioprostheses may develop obstruction, likewise due either to wear-and-tear degeneration or infection.
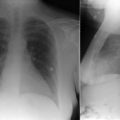
Mechanical prostheses rarely develop significant transvalvar insufficiency but often develop paravalvar insufficiency, which may be sterile, but usually is due to infection, and often includes dehiscence ( Figs. 12-2 and 12-3 ). Obstruction of a mechanical prosthesis may occur because of thrombosis, pannus (fibrous scar tissue) ingrowth, both conditions, or, rarely, to infection with large vegetations ( Figs. 12-4 to 12-7 ).
All mechanical prostheses are apparent on chest radiograph. Most, but not all, bioprostheses are radiographically apparent. Prior sternotomy wires may be the only sign of prior stentless bioprosthesis insertion. For now, all percutaneously or transapically inserted aortic valve bioprostheses are radiographically apparent.

Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


