16 Pulmonary Valvar Stenosis
With Christian J. Kellenberger
Definition and Classification
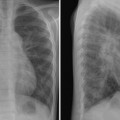
 Pulmonary valvar stenosis occurs with a reduced orifice of the pulmonary valve due to fusion of the thickened valve leaflets. The valve can also be bicuspid and have a hypoplastic annulus. Stenosis of the dysplastic valve is typically seen in Noonan syndrome.
Pulmonary valvar stenosis occurs with a reduced orifice of the pulmonary valve due to fusion of the thickened valve leaflets. The valve can also be bicuspid and have a hypoplastic annulus. Stenosis of the dysplastic valve is typically seen in Noonan syndrome.
 Isolated or associated with subvalvar, supravalvar, or peripheral branch pulmonary artery stenosis
Isolated or associated with subvalvar, supravalvar, or peripheral branch pulmonary artery stenosis
 Critical pulmonary stenosis refers to obstruction resulting in suprasystemic right ventricular systolic pressures, tricuspid regurgitation, and a right-to-left shunt across the atrial septum, and often pulmonary circulation is dependent on the flow through the ductus arteriosus.
Critical pulmonary stenosis refers to obstruction resulting in suprasystemic right ventricular systolic pressures, tricuspid regurgitation, and a right-to-left shunt across the atrial septum, and often pulmonary circulation is dependent on the flow through the ductus arteriosus.
Pathophysiology
 Increased impedance to right ventricular outflow requires increased right ventricular pressure to maintain pulmonary circulation.
Increased impedance to right ventricular outflow requires increased right ventricular pressure to maintain pulmonary circulation.
 Increasing pressure results in concentric hypertrophy of the right ventricle and loss of compliance with impaired diastolic filling.
Increasing pressure results in concentric hypertrophy of the right ventricle and loss of compliance with impaired diastolic filling.
 Systolic pressure in the right ventricle and degree of hypertrophy are proportional to the degree of obstruction in the absence of heart failure.
Systolic pressure in the right ventricle and degree of hypertrophy are proportional to the degree of obstruction in the absence of heart failure.
 Severity of the lesion is generally classified according to the right ventricular systolic pressure.
Severity of the lesion is generally classified according to the right ventricular systolic pressure.
 Less severe obstruction is well tolerated with gradual hypertrophy and dilatation of the right ventricle and preserved right ventricular function.
Less severe obstruction is well tolerated with gradual hypertrophy and dilatation of the right ventricle and preserved right ventricular function.
 More severe obstruction leads to suprasystemic right ventricular pressures, moderate dilatation of the right ventricle, and right heart failure.
More severe obstruction leads to suprasystemic right ventricular pressures, moderate dilatation of the right ventricle, and right heart failure.
 Right atrium may also become hypertrophied and dilated with tricuspid valve regurgitation.
Right atrium may also become hypertrophied and dilated with tricuspid valve regurgitation.
 Increasing right atrial pressures leads to right-to-left shunting at atrial level if foramen ovale is patent or an atrial defect is present.
Increasing right atrial pressures leads to right-to-left shunting at atrial level if foramen ovale is patent or an atrial defect is present.
Clinical Manifestations