Fig. 38.1
MRI sagittal STIR of a hindfoot coalition of the calcaneus and navicular with a stress response

Fig. 38.2
X-ray showing a hallux valgus
38.2 Mechanisms of Injury
38.2.1 Acute Injuries
38.2.1.1 Fractures
Common fractures in the athlete include avulsion of the proximal end of the fifth metatarsal, which is secondary to a traction injury caused by the peroneus brevis. This lesion must be distinguished from a normal apophysis, which occurs in this location in adolescence (Fig. 38.3a, b). The apophysis has its alignment parallel to the shaft of the metatarsal, whilst the fractures are closer to 90° to the axis of the metatarsal. Considerable confusion may occur when there is an avulsion of the apophysis in a young athlete or if there is a fracture through the apophysis. In these circumstances, imaging is of considerable importance, as it will detect the bone oedema and also the fracture margins.
Fig. 38.3
(a) X-ray showing a fracture of the base of the fifth metatarsal. (b) X-ray showing a fifth toe apophysis
An avulsion fracture of the base of the fifth metatarsal has to be distinguished from Jones’ fracture (also called dancer’s fracture) that is located more distally with transverse course at the proximal diaphyseal or metaphyseal area. This fracture may be related to acute ankle inversion trauma but also to stress from running (fatigue fracture) or osteopenia (insufficiency fracture). Jones fractures unlike avulsion fractures are prone to delayed and even non-union and often need operative intervention (Jones 1902).
Fractures of all the tarsal bones and metatarsals may occur as an acute event. Midfoot injuries are often the result of stamping by another athlete. The fractures seen are identical to those that occur in nonathletes. Avulsion of the medial border of the os naviculare by the tibial posterior insertion is a potential adolescent or children’s injury. This must be distinguished from a secondary ossification centre occurring at this site. Some would argue that the so-called os naviculare is an old avulsion injury. Those with a secondary ossification centre or a normal variant at this location tend to be at greater risk of avulsion displacement, and, therefore, pain in the region of an apparently normal variation should be considered seriously and investigated further when the clinical symptoms suggest that this is the location of the pain (Mellado et al. 2003; Tuthill et al. 2014) (Fig. 38.4).
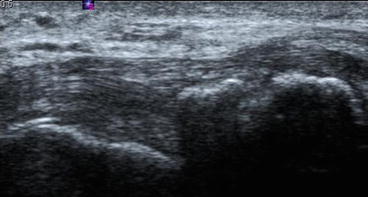
Fig. 38.4
Ultrasound showing the distal insertion of the tibialis posterior tendon and an os naviculare
38.2.1.2 Ligament Tears
Specific ligamentous or capsular injury is the condition termed “turf toe” (Clanton and Ford 1994). This is an avulsion or traction injury of the plantar plate most typically of the great toe but also rarely seen in other toes. This is associated with the use of soft and flexible footwear whilst competing on artificial turf. The sudden deceleration of the foot with hyperextension can lead to an avulsion injury where the plantar plate is detached from its normal insertion (Fig. 38.5). This condition can range from an enthesopathy with flexor tendon thickening to tears of the plantar plate, metatarsal-sesamoid ligament and/or inter-sesamoid ligament and, in the worst case, to complete avulsion of the insertions with or without associated osseous or cartilage injury. There will be localised pain, tenderness, dysfunction and oedema. This injury may lead to chronic problems if not properly treated in the early stages (Allen et al. 2004). Other ligament injuries may occur in the midfoot particularly in the intertarsal and tarsometatarsal ligaments (Lisfranc and Chopart). The spring ligament has been dealt with in the ankle chapter.
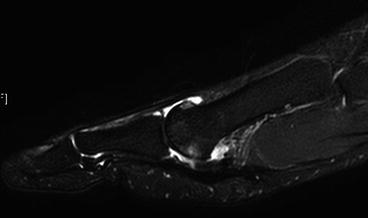
Fig. 38.5
MRI sagittal PDFS showing a plantar plate injury
38.2.1.3 Tendon Injuries
The distal portions of the tendon of tibialis posterior, tibialis anterior, flexor digitorum longus and the peroneal tendons are subject to chronic tendinopathy. The nature of which will depend upon the precipitating mechanism. Thickening of the tendon, tendon sheath fluid and paratenon oedema are all features. Delamination may occur in the tendon itself and enthesopathy at its insertion. These may be relatively acute injuries with avulsion and rupture. Chronic tendinopathy is dealt with later in this section. Avulsion injuries of the tendons in the feet may lead to considerable retraction at the tendon ends. Extensor tendon injuries are less common although the tibialis anterior may be affected by impaction against the anterior part of the footwear.
38.2.1.4 Muscle Injury
Although these are rare in the athlete, unusual injuries can occur due to a direct blow or a sudden change of direction of the foot (Fig. 38.6) (MRI of foot muscle injury).
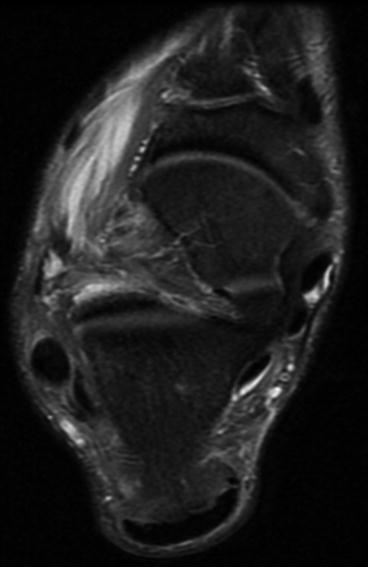
Fig. 38.6
MRI of a foot muscle injury – extensor hallucis brevis
38.2.2 Chronic Injuries
38.2.2.1 Stress Injuries
Stress (fatigue and insufficiency) injuries occur in the foot due to repetitive activity. There are precipitating factors: particularly congenital, deformity and previous fracture.
The stress response in bone will start as bone oedema. Next, periosteal oedema and then periosteal new bone formation may occur. Eventually, thickening of the cortex and the type of the stress injury with separation and full fracture may also occur. If patients rest and remove the load to the bone, then the fractures will heal spontaneously with initial resorption and then sclerosis as part of the bone repair process. There will be localised cortical thickening which in time will remodel. As athletes often return to physical activity too early in the stage of healing, secondary new bone formation periosteal response is sometimes seen in healed or partly healed fractures. Therefore, any stage of the oedema, periosteal response and bone defects may be seen in combination. Stress injuries may occur in the midfoot, particularly in people with hindfoot or midfoot deformity which may also occur in any of the bones (Dixon et al. 2011) (Figs. 38.7, 38.8, and 38.9).
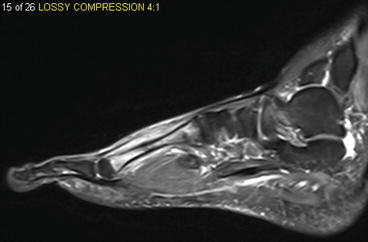
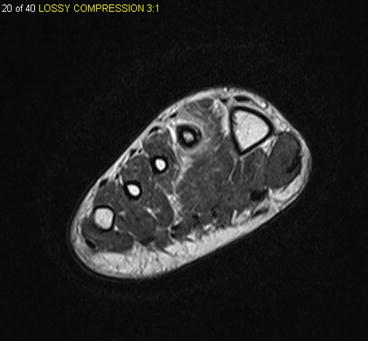
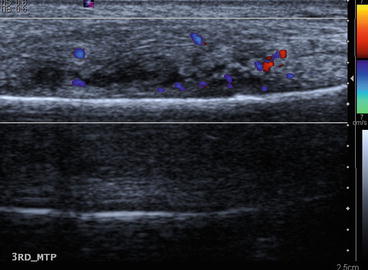
Fig. 38.7
MRI STIR sequence sagittal of a second metatarsal stress fracture
Fig. 38.8
MRI STIR sequence axial of a second metatarsal stress fracture
Fig. 38.9
US with colour Doppler of a third metatarsal stress fracture
38.2.2.2 Tendinopathy
In chronic tendinosis, delamination is more common, with swelling of the tendon, which leads to thickening and increased water content on imaging and neovascularisation of the tendon. The most common tendons in the feet are the tibialis posterior, peroneus tendons and tibialis anterior tendons (Fig. 38.10).
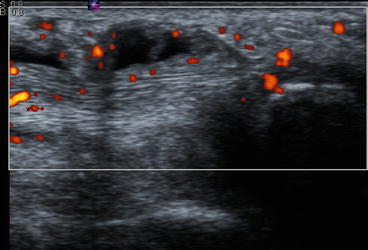
Fig. 38.10
Ultrasound showing the distal insertion of the tibialis posterior tendon with tenosynovitis and neovascularisation
38.2.2.3 Enthesopathy
A traction injury at the tendon insertion, or enthesis, will lead to oedema, swelling and thickening of the enthesis and distal tendon, small collections of adjacent fluid and neovascularity both within the tendon and the adjacent tissues. Enthesitis or traction bony spurs may occur with associated underlying bone oedema. Common sites for enthesopathy are at the insertion of the Achilles, tibialis posterior on the navicular bone and at the insertion of the peroneus brevis on the fifth metatarsal bone.
38.3 Plantar Fascia
Plantar fascia is a fan or tree-like structure which extends from its root in the calcaneus to the insertion of the fascia on the anterior part of the foot where it is spread out in a lateral and medial direction. Conditions which affect the plantar fascia in athletes include rupture of the fascia, chronic traumatic or overuse fasciitis and traction enthesopathy at the plantar fascia insertion in the calcaneus. Patients with plantar fibromas or contractures (Lederhosen disease) may present in an athletic environment although this is an intrinsic genetic disorder.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


