Abstract
The future of PET lies in the potential for multiple clinically valuable radiotracers other than FDG. This chapter discusses the basics of five additional clinically valuable PET radiotracers: 18F-sodium fluoride, 18F-FACBC, 11 C-choline, 68 Ga-DOTATATE, and 68 Ga-PSMA-11.
Keywords
FDG, PET/CT, sodium fluoride, FACBC, fluciclovine, choline, DOTATATE, PSMA
The development and use of positron emission tomography (PET) radiotracers has tremendous potential for the advancement of oncologic imaging. There has been preclinical development on hundreds of PET radiotracers, and the most promising have advanced into clinical trials. As of 2018 the US Food and Drug Administration (FDA) has approved five PET radiotracers which are used for oncologic imaging:
- 1.
18F-fluorodeoxyglucose (FDG)
- 2.
18F-sodium fluoride (Na18F)
- 3.
18F-anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (18F-FACBC, also known as fluciclovine and by the brand name Axumin)
- 4.
11 C-choline
- 5.
68 Ga-DOTA-octreotate ( 68 Ga-DOTATATE, also known by the brand name NETSPOT)
This brief introduction is not intended to help master these complex PET/CT radiotracers, each of which could be the basis of its own textbook. Rather, this is to demonstrate the versatility of PET/CT as a platform for the development of novel imaging studies. Although it is common to hear clinicians discuss ordering a “PET/CT,” they are actually ordering an FDG PET/CT, a Na18F PET/CT, or a 68 Ga-DOTATATE PET/CT. Each study has its own uses, advantages, and limitations.
18F-Sodium Fluoride (Na18F)
Intravenous administration of Na18F leads to incorporation of 18F into bone at sites of altered osteogenesis. Because tumors involving the bone often lead to altered osteogenesis, Na18F can be used to detect malignancy involving the bone. Na18F was approved by the FDA in 1972 and became the first “bone scan” for detection of osseous metastases in the 1970s. The development of less expensive Tc-99m pertechnetate (99mTc)-labeled bisphosphonate agents and Anger gamma cameras optimized for imaging the 140-KeV photons from 99mTc led to Na18F bone scans being replaced by 99mTc radiotracers such as Tc-99m medronate (MDP). Decades later, the development of PET and then PET/CT scanners has led to resurgence in the use of Na18F bone scans. Na18F PET/CT allows for higher spatial resolution and improved image quality compared with MDP planar and single-photon emission computed tomography (SPECT)/CT imaging. Na18F also has higher lesion-to-background signal and more rapid blood clearance than does MDP, allowing for shorter tracer injection to scanning times. These technical advantages have clinical implications because Na18F PET/CT has been shown to have greater sensitivity and specificity for the detection of osseous metastases than does MDP imaging. The major drawbacks of Na18F PET/CT are cost, given that MDP can be performed inexpensively, and radiologist time, because interpretation of the thousands of images in a Na18F PET/CT takes significantly longer than most MDP studies.
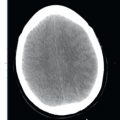
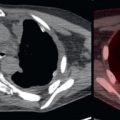
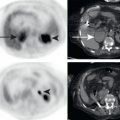
Because Na18F targets sites of osteogenesis, the skeleton is the dominate finding on a normal Na18F study ( Fig. 24.1 ). Na18F is excreted by the kidneys, thus the kidneys, ureter, and bladder may be visualized. In contrast to FDG, which accumulates in the tumor itself, it is important to recognize that Na18F does not image the tumor itself but rather the osteogenic reaction to tumor causing bone destruction (you image the bone, not the tumor). The osteogenic reaction to tumor may be substantial, and thus Na18F may demonstrate extensive osseous malignancy ( Fig. 24.2 ). Depending on the extent of the osteogenic reaction and the metabolism of the tumor, more osseous metastases may be visualized by Na18F than by FDG. Unfortunately, many benign processes also elicit osteogenesis. Na18F uptake will be seen at sites of arthritis, trauma, and metabolic abnormalities, as well as at areas of bone remodeling caused by Paget disease and fibrous dysplasia and by benign bone tumors such as osteoid osteomas. Benign processes may be more Na18F avid than malignancies; thus the standardized uptake value (SUV) cannot reliably differentiate benign from malignant processes. The morphology of the Na18F avidity, such as linear avidity at vertebral endplates, may help to classify uptake as degenerative and thus benign. Often, the corresponding CT images will help to distinguish benign from malignant Na18F avidity ( Fig. 24.3 ). In general, Na18F foci within the bone, not associated with the joint surface, and without a benign correlate on CT (such as fracture, degenerative changes, or benign bone tumor), are suspicious for osseous malignancy.



Because you are imaging the bone, not the tumor, increasing Na18F avidity following therapy presents a conundrum. Just as increasing MDP avidity following therapy may represent either increasing metastases or decreasing metastases with “flare response” from osseous healing, the same can be seen with Na18F.
68 Ga-DOTATATE
Neuroendocrine tumors (NETs) arise from cells of the nervous and endocrine systems. They are most common in the small bowel, pancreas, and lung. They may also be found in the thyroid, thymus, pituitary, adrenal gland, and many other organs. Small bowel and lung NETs are often referred to as carcinoids. NETs of the pancreas arise in the pancreatic islet cells. Merkel cell carcinomas are a NET of the skin. Pheochromocytomas/paragangliomas are NETs of the adrenal glands and sympathetic nervous system. These diverse neoplasms share common features, such as production of polypeptide hormones and expression of somatostatin receptors (SSTRs).
There are multiple radiotracers that target SSTRs, allowing for SSTR imaging. 68 Ga-DOTATATE is a molecule that predominantly targets SSTR2, radiolabeled with the positron emitter 68 Ga. In 2016 the FDA approved 68 Ga-DOTATATE for PET localization of SSTR-positive NETs. Well-differentiated NETs often express relatively high levels of SSTR and are 68 Ga-DOTATATE avid. Poorly differentiated NETs often lose SSTR expression and are not well imaged by 68 Ga-DOTATATE. Poorly differentiated NETs may have high metabolism and be visualized by FDG. Thus well-differentiated NETs are often well visualized by 68 Ga-DOTATATE but poorly visualized by FDG, whereas poorly differentiated NETs demonstrate the reverse imaging characteristics. Of course, there is a spectrum of 68 Ga-DOTATATE and FDG avidity among NETs, and some may be visualized by both radiotracers or by neither.
SSTR imaging with 68 Ga-DOTATATE PET/CT has been found to be more sensitive than SSTR imaging with 111 indium-penteoctreotide (Octreoscan), as well as anatomic imaging with magnetic resonance (MR) or CT for the detection of many primary and metastatic NETs. 68 Ga-DOTATATE PET/CT is also superior to Octreoscan SPECT/CT due to improved image quality and spatial resolution, reduced patient radiation dose, and the ability to perform same day imaging. Given the many strengths of 68 Ga-DOTATATE PET/CT, it is likely to increasingly replace Octreoscan SPECT/CT for imaging of NETs.
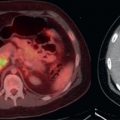
Physiologic 68 Ga-DOTATATE avidity is found in multiple organs which express SSTR ( Fig. 24.4 ). Intense 68 Ga-DOTATATE signal is seen in the spleen and kidneys, with somewhat less intense uptake in the liver. The pituitary, salivary, thyroid, and adrenal glands are also often 68 Ga-DOTATATE avid. The bladder may be seen due to renal excretion. The pancreas may contain areas of 68 Ga-DOTATATE avidity, particularly in the uncinate process, and this avidity may be confused with neoplasm.