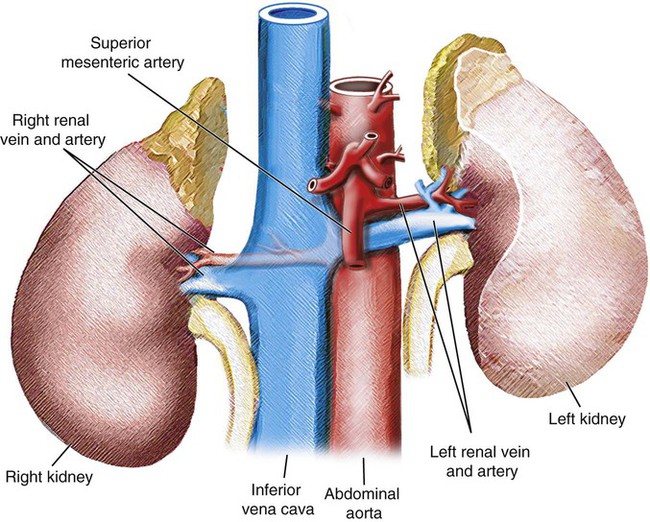
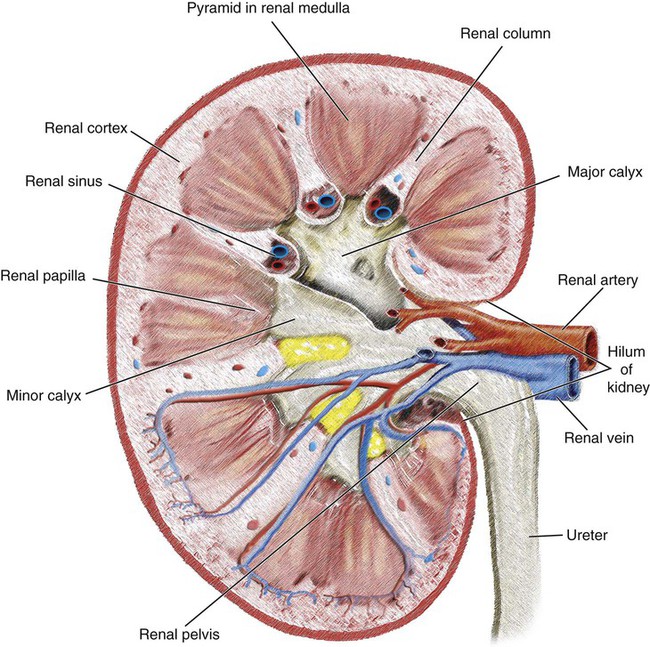
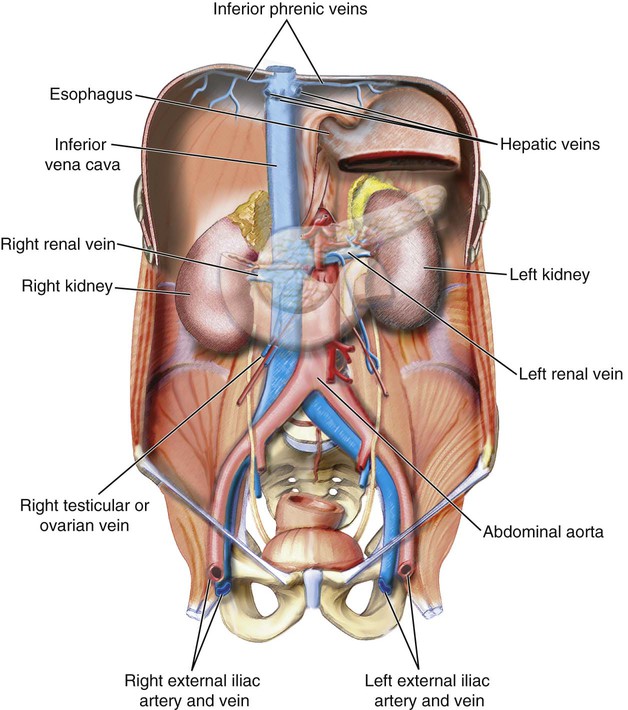
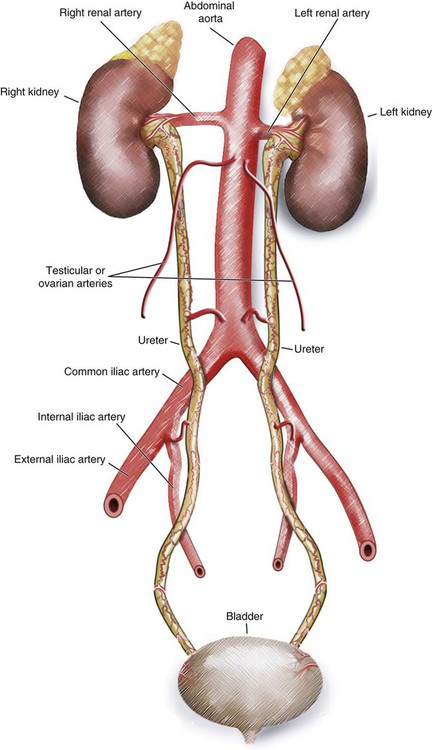
Chapter 57 Nadia J. Khati, Morvarid Alaghmand, Ali Noor, Aaron Reposar, Rishabh Chaudhari, Ramy Khalil and Anthony C. Venbrux The renal artery originates from the aorta at the area between L1 and L2, just inferior to the origin of the superior mesenteric artery (SMA). These arteries are typically posterior to the renal veins and anterior to the renal pelvis. The left renal artery arises at a higher level than the right renal artery and follows an upward course, but the right one is longer and passes posterior to the vena cava, with a downward course to the right kidney (Fig. 57-1). As each renal artery approaches the hilum, it divides into anterior and posterior segmental arteries (Fig. 57-2). The posterior branch, which arises first, supplies a large portion of the posterior part of the kidney. Next, the four anterior divisions at the renal hilum arise as apical, upper, middle, and lower anterior segmental arteries. The apical and lower anterior divisions supply the anterior and posterior surfaces of the upper and lower renal poles. The upper and middle divisions supply the remaining parts of the anterior surface. The other divisions after the segmental arteries are the lobar, interlobar, arcuate, intralobular, and glomerular arteries. The renal artery gives off small branches to the renal capsule and adrenal gland (inferior adrenal artery). As mentioned earlier, the renal veins are anterior to the renal arteries (see Fig. 57-1). The left renal vein is longer and crosses the midline anterior to the abdominal aorta and posterior to the SMA. This vein receives the left testicular or ovarian vein from below, the left suprarenal vein from above, and the lumbar vein before joining to the inferior vena cava (IVC; Fig. 57-3). As the ureters pass toward the bladder, they receive branches from adjacent vessels (Fig. 57-4). The renal arteries supply the upper end of the ureters, abdominal aorta, and testicular or ovarian arteries. The common iliac arteries supply the middle part, and the rest are supplied by branches from internal iliac arteries. There is anastomosis between these branches.
Renal Vasculature
Renal Vascular Anatomy
Arterial Supply
Venous System
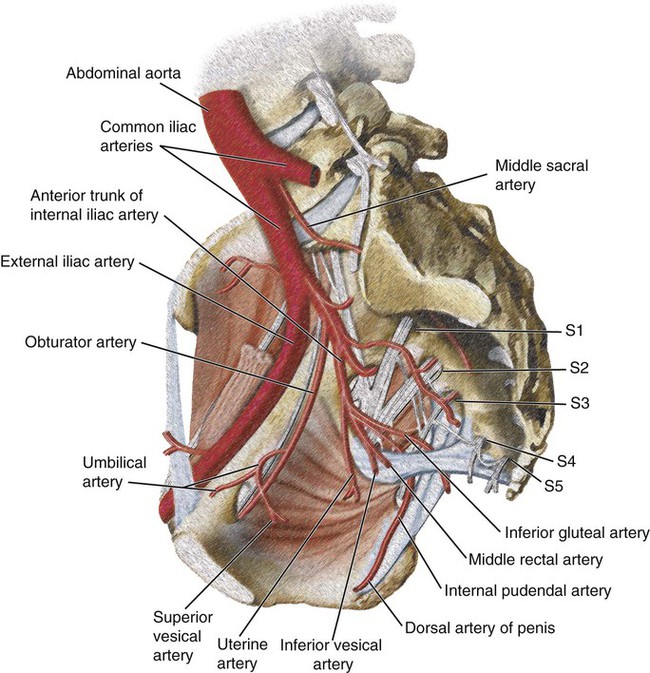
Ureteric Vasculature
Radiology Key
Fastest Radiology Insight Engine