Chapter 11 Secondary Intraparenchymal Hemorrhages
Multiple causes other than hypertension may provoke intraparenchymal hematomas. Recognizing them may be difficult, especially in the acute phase. However, some of these causes must be promptly identified to avoid devastating complications. Hemorrhages induced by excessive anticoagulation and those produced by bleeding vascular anomalies are examples of highly dangerous situations that demand immediate therapeutic intervention.
Brain imaging is particularly valuable in the distinction of secondary causes of intraparenchymal hematoma (Table 11-1). Radiological hints are frequently subtle but quite reliable. Imaging often provides the first, and sometimes only evidence that a secondary cause is responsible for the hemorrhage. Throughout this chapter we attempt to summarize useful discriminating signs as we present examples of the most common secondary causes of intraparenchymal bleeding.
TABLE 11-1 Secondary causes of intraparenchymal hemorrhage
| Cerebral amyloid angiopathy |
| Hemorrhagic transformation of ischemic infarction |
| Anticoagulation |
| Thrombolysis |
| Intrinsic coagulation disorders |
| Sympathomimetic drugs (cocaine, amphetamines, decongestants, anorectics) |
| Infective endocarditis |
| Vasculitis |
| Moyamoya disease |
| Neurosurgical and neuroendovascular procedures |
| Cerebral venous thrombosis |
| Vascular anomalies |
| Saccular aneurysms |
| Arteriovenous malformations |
| Cavernous malformations |
| Dural arteriovenous fistulas |
| Tumors (primary or metastatic) |
| Head trauma |
CEREBRAL AMYLOID ANGIOPATHY
Cerebral amyloid angiopathy (CAA) is characterized by the accumulation of amyloid β and other amyloidogenic peptides in the walls of medium and small cortical and leptomeningeal vessels leading to vascular fragility and probably dysfunction.1,2 Amyloid deposition and hemorrhage are favored by the presence of APOE  2 and
2 and  4 alleles,3 and vascular amyloid deposits are often (but not always) seen in combination with changes of Alzheimer’s disease.4 The restricted location of the deposits explains why hemorrhages are always lobar and involve the cortex of the brain (or, much less commonly, the cerebellum). It may account for more than one third of cases of lobar intracerebral hemorrhage (ICH) in the elderly population (age > 65 years).5,6 The prevalence of CAA in brain-bank studies exceeds 50% in patients over age 70,7 and it is severe in more than 10% of patients over age 80.8 Thus the incidence of CAA-related hemorrhages is likely to continue to increase substantially with the aging of the population.
4 alleles,3 and vascular amyloid deposits are often (but not always) seen in combination with changes of Alzheimer’s disease.4 The restricted location of the deposits explains why hemorrhages are always lobar and involve the cortex of the brain (or, much less commonly, the cerebellum). It may account for more than one third of cases of lobar intracerebral hemorrhage (ICH) in the elderly population (age > 65 years).5,6 The prevalence of CAA in brain-bank studies exceeds 50% in patients over age 70,7 and it is severe in more than 10% of patients over age 80.8 Thus the incidence of CAA-related hemorrhages is likely to continue to increase substantially with the aging of the population.
The definitive diagnosis of CAA requires pathological demonstration. However, in practice this is rarely feasible or justified. Criteria have been designed to make the diagnosis of possible or probable CAA based solely on clinical and radiological data.9 Possible CAA requires CT or MRI evidence of a single lobar ICH in a patient 55 years or older with no other cause for the hemorrhage. When there is clinicoradiological evidence of two or more lobar cerebral or cerebellar hemorrhages in a patient 55 years or older with no other causes for the lesions the diagnosis is probable CAA.
These criteria focus on the identification of cases of lobar ICH that can only be attributed to CAA. However, CAA may also play a role in the genesis of lobar hematomas in patients with coexistent causes. In fact, it has been shown that CAA increases the risk of intracranial bleeding in patients receiving anticoagulants10 and thrombolytic agents.11
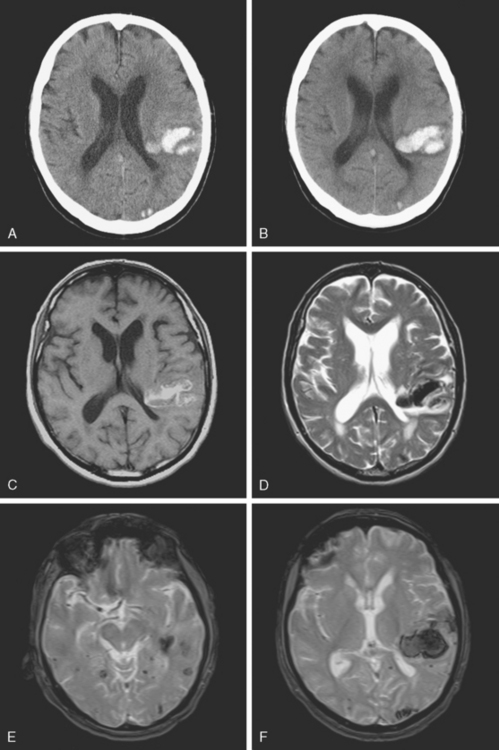
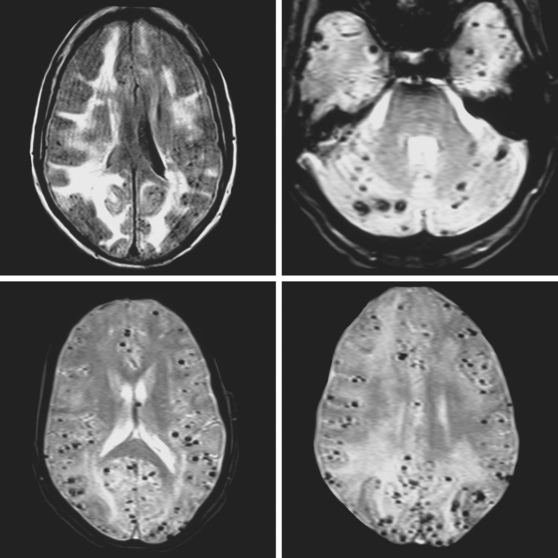
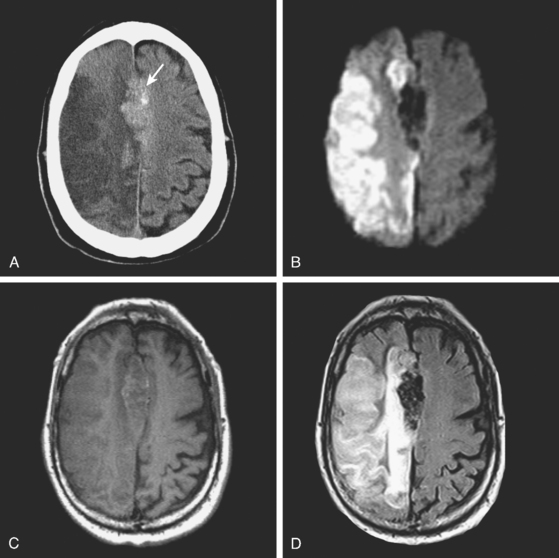
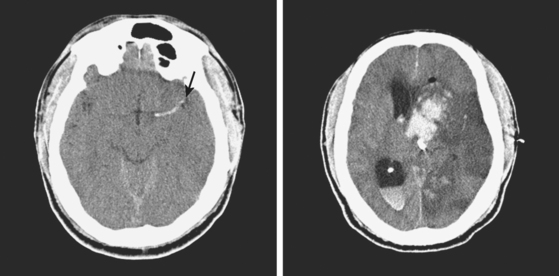
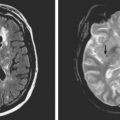
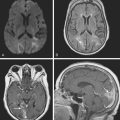
A 73-year-old man without previous known illnesses was brought to the emergency department by his son for evaluation of acute speech changes. On physical examination, the patient was fully awake and had fluent dysphasia without associated motor or sensory deficits. Head CT scan disclosed a left parietal hemorrhage of moderate volume (Figure 11-1). When specifically questioned, the patient’s son acknowledged that he had noticed subtle changes in the behavior of his father over the previous year. His memory had been declining for a longer time. Brain magnetic resonance imaging (MRI) revealed multiple cortical microhemorrhages, supporting the clinical suspicion of cerebral amyloid angiopathy. The patient developed episodes of agitation during the hospitalization and only achieved minimal recovery from his dysphasia.
HEMORRHAGIC TRANSFORMATION
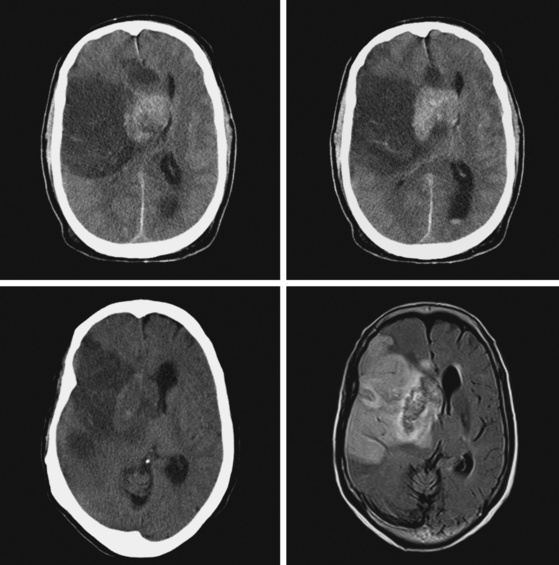
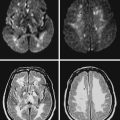
An 86-year-old woman with history of hypertension and right parietal meningioma was found unresponsive on her bed during a cruise. She was intubated and emergently transferred to our hospital for evaluation. On arrival, she was drowsy, globally aphasic, and had flaccid right hemiplegia. Her pulse was irregularly irregular, and electrocardiogram confirmed the diagnosis of atrial fibrillation. Initial CT scan is shown in Figure 11-4, A and B.
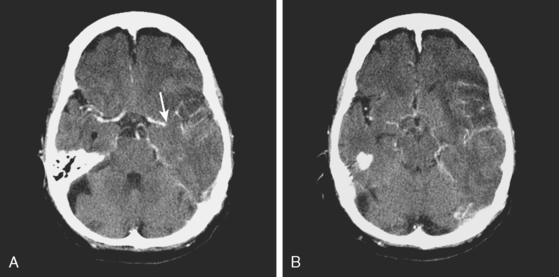
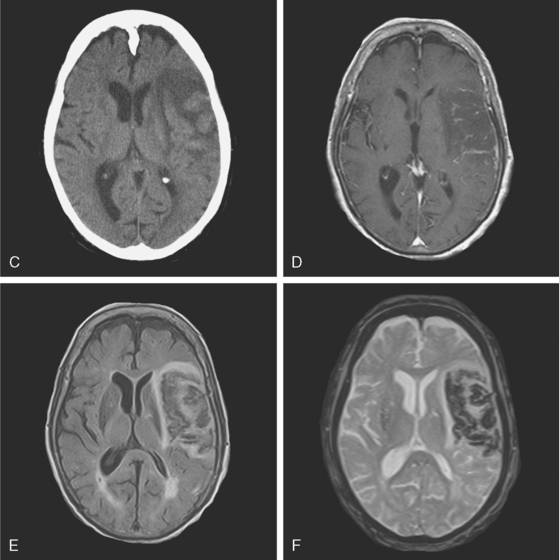
CT scan of the head and brain MRI obtained 48 hours after symptom onset showed evidence of hemorrhagic transformation (Figure 11-4, C–F). The patient had been taking aspirin before the stroke, and 325 mg of aspirin had been administered since admission. Anticoagulation had not been initiated because of the perceived high risk of hemorrhagic conversion of the ischemic infarction. On the third day after stroke onset, the patient’s neurological status deteriorated because of progression of mass effect. She responded favorably to treatment with mannitol. Her subsequent clinical course was complicated with the development of acute renal failure, congestive heart failure, bilateral pneumonia, and sepsis. She required tracheostomy and was eventually transferred to a nursing home in fair condition. Six months later, she had improved communication abilities but remained functionally dependent.
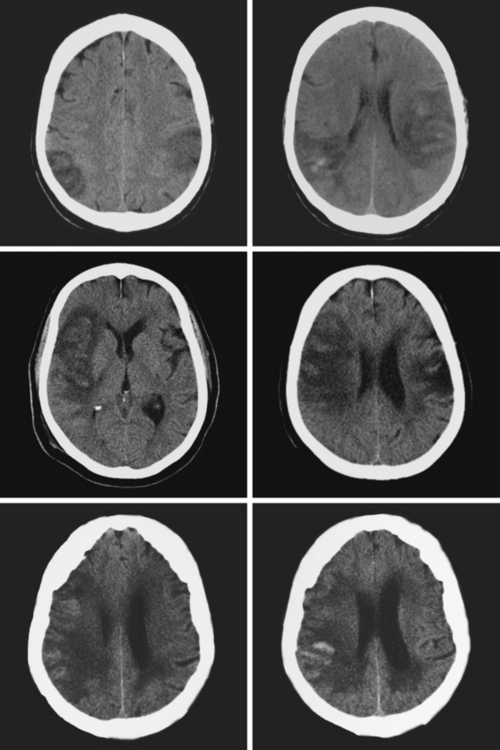
Figure 11-5 Multiples examples of hemorrhagic conversion of ischemic infarctions on head computed tomography scans.
HEMORRHAGIC COMPLICATIONS OF THROMBOLYSIS
Intracranial hemorrhage is the most feared complication of thrombolysis. Symptomatic hemorrhagic transformation occurs in 6% to 7% of patients who receive treatment with recombinant tissue plasminogen activator (rt-PA) within 3 hours of symptom onset.17,18 The rate of hemorrhage is about 10% after intra-arterial lysis.19 Hemorrhagic risks with combined intravenous–intra-arterial lysis20 and mechanical embolectomy21 also fall within this range. It tends to occur early after infusion of rt-PA and carries high mortality. However, it does not negate the value of thrombolysis in appropriate candidates for this acute intervention.
Clinical factors include older age, pretreatment hypertension, pretreatment hyperglycemia, history of diabetes mellitus, use of antiplatelets other than aspirin before stroke onset, greater stroke severity (i.e., higher score on the National Institutes of Health stroke scale) at baseline, and higher blood pressure over the first 24 hours after lysis.22–26 Radiological predictors on initial CT scan include hypodense lesion greater than one third of MCA territory and hyperdense MCA sign.22,23 MRI with diffusion-weighted imaging/perfusion-weighted imaging (DWI/PWI) may be particularly useful because very low initial apparent diffusion coefficient (ADC) values, persistent perfusion deficits on PWI, and very large areas of restricted diffusion on DWI strongly correlate with heightened risk of hemorrhagic transformation.22,27–31 Although DWI and PWI are not usually available when thrombolysis is administered within the 3-hour window, the predictive information provided by these sequences may become important if thrombolysis is considered at later times in patients with persistent radiological penumbra. Leukoaraiosis has also been associated with increased risk of ICH after thrombolysis.32 However, the presence of cerebral microhemorrhages seen on T2* sequence does not appear to influence substantially the risk of symptomatic ICH.33 Although the factors influencing the risk of hemorrhage after intra-arterial thrombolysis or multimodality therapy have been less studied, available evidence indicates that they do not differ significantly from those that determine the risk after intravenous lysis.34,35
It has been appropriately postulated that the deleterious consequences of symptomatic ICH after thrombolysis may have been overestimated by failing to consider the predicted outcome at the time of initial assessment in patients who subsequently had symptomatic ICH.36 Because outcome in many of these patients is anticipated to be poor (because of older age, more severe deficits, and larger strokes), when the predicted functional outcome is compared with the actual outcome after ICH, the number necessary to harm for intravenous thrombolysis turns out to be much smaller than commonly thought. In other words, symptomatic ICH after thrombolysis may further worsen outcome in patients with poor chances of recovery without thrombolysis, but it rarely causes devastating damage in patients with better anticipated outcome at the time of treatment.
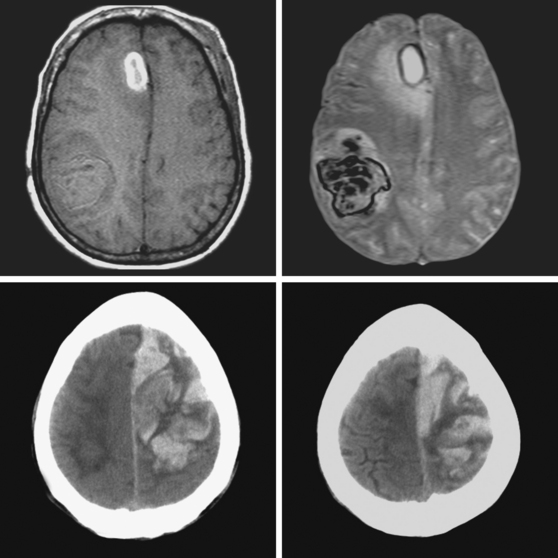
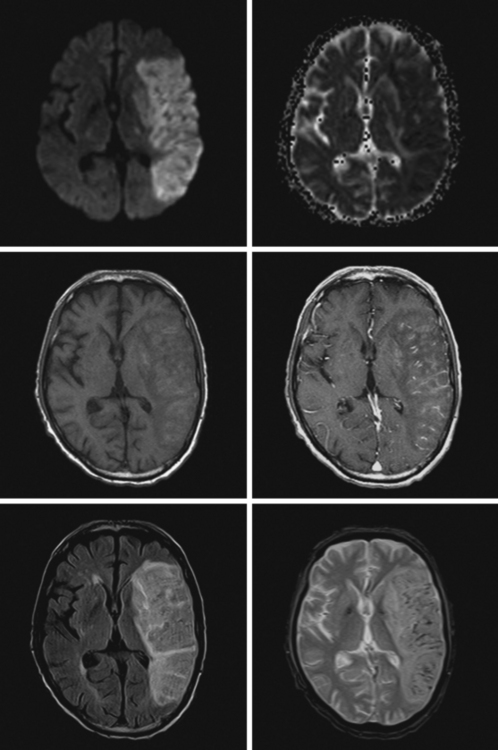
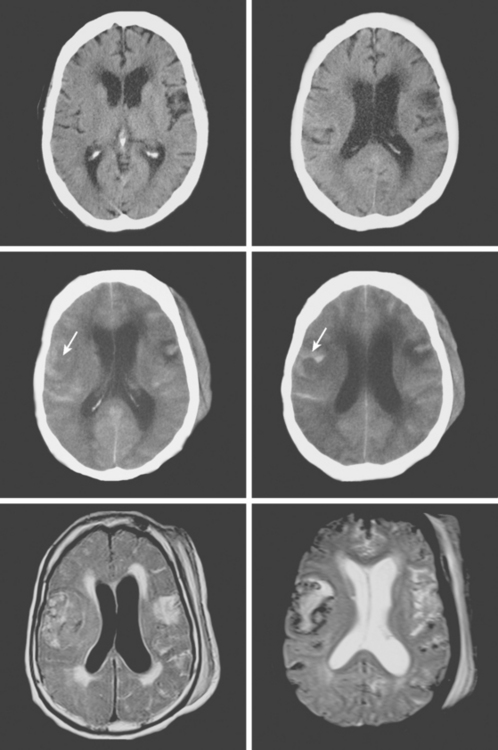
A 68-year-old man with previous history of a left hemispheric stroke presented to the emergency department with sudden onset of left-sided weakness within 2 hours of symptom onset. Examination revealed right gaze preference, left homonymous hemianopia, left hemiparesis, and partial left hemibody neglect. Initial CT scan is shown in Figure 11-10 (upper row). He had no contraindications for intravenous thrombolysis and consequently received rt-PA with the bolus given 2 hours and 45 minutes after instauration of deficits. Three hours later, the patient was noticed to be somnolent, and his weakness had worsened to the point of hemiplegia. Emergent repeat CT scan displayed intraparenchymal and subarachnoid hemorrhage (Figure 11-10, middle row). He was treated with fresh frozen plasma and cryoprecipitate. Although his deficits remained severe, he subsequently improved. Brain MRI on day 5 showed the hemorrhagic transformation of his right MCA infarction with mild regional mass effect (Figure 11-10, lower row).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


