SECTION XI THORACIC IMAGING
Essentials 1
Case
An asymptomatic 23-year-old foreign exchange student presents with a required health clearance chest radiograph.

Questions
1. What is the next MOST reasonable course of action?
A. Additional radiographic views
B. Magnetic resonance imaging of the chest
C. Treatment with antibiotics
D. No further action
E. Computed tomography of the chest
2. What is the MOST likely diagnosis?
A. Pectus excavatum
B. Right middle lobe pneumonia
C. Right lower lobe pneumonia
D. Right hilar mass
E. Cardiophrenic angle mass
3. Regarding the diagnosis, which ONE of the following is correct?
A. A familial occurrence is reported in 70% of cases.
B. The condition is associated with Down syndrome.
C. There is a female predominance (female-to-male ratio of 3:1).
D. Tricuspid regurgitation is reported in 20 to 60% of cases.
E. Pectus patients may have an abnormal Haller index.
Answers and Explanations
Question 1
D. Correct! No further action is needed. The two-view chest confirms a pectus excavatum deformity. In most pectus patients (including the test patient), the abnormality is mild and clinically insignificant. When severe, however, a pectus excavatum deformity can cause pain the chest and back and even impair cardiac and respiratory function. In select symptomatic cases, cross-sectional imaging treatment is sometimes performed.
Other choices and discussion
A. Additional radiographic views are occasionally used to better localize pathology or to differentiate a real finding from overlapping normal tissue. In this case, as the two-view chest successfully excludes a nodule/infiltrate and clearly demonstrates the sternal depression, more views are not required.
B. Additional cross-sectional imaging is not required at this point. The lateral chest radiograph clearly demonstrates the pectus excavatum deformity, and there is no lung or mediastinal abnormality seen on the lateral view.
The most common indications for magnetic resonance imaging of the chest include the assessment of cardiac morphology and function, aortic dissection, pleural and mediastinal masses, and pericardial disease.
C. The patient is asymptomatic and there is no lung consolidation seen on the lateral view, so antibiotic treatment is not indicated.
E. Additional cross-sectional imaging is not required at this point. Computed tomography may be indicated eventually in treatment planning for severe cases, but is not needed for the initial diagnosis.
Question 2
A. Correct! The lateral radiograph demonstrates inward displacement of the sternum. This confirms a pectus excavatum deformity, which is a congenital deformity of the anterior thoracic wall in which the sternum has a caved-in or sunken appearance. The depressed sternum replaces aerated lung at the right heart border, and the right heart border appears to be obscured.
Pectus carinatum, also called pigeon chest, is a deformity of the chest characterized by a protrusion of the sternum and ribs.
The other choices are all incorrect. There is no pneumonia, consolidation, or mass, because the lateral view excludes those findings and confirms the pectus deformity.
Question 3
E. Correct! The Haller index is the ratio of the transverse diameter (the horizontal distance of the inside of the ribcage) to the anteroposterior diameter (the shortest distance between the vertebrae and sternum). A normal Haller index is 2.5. A significant pectus excavatum has an index > 3.25.
Other choices and discussion
A. A familial occurrence of pectus deformity is reported in 35% of cases.
B. Pectus deformity can be with Marfan syndrome, Poland syndrome, Noonan syndrome, Ehlers-Danlos syndrome, neurofibromatosis type I, and osteogenesis imperfecta.
C. There is a male predominance (male-to-female ratio of 3:1).
D. Mitral valve prolapse (not tricuspid regurgitation) has been reported in 20 to 60% of cases.
Suggested Readings
Dähnert W. Radiology Review Manual. Philadelphia, PA: Lippincott Williams & Wilkins; 2007 Mak SM, Bhaludin BN, Naaseri S, Di Chiara F, Jordan S, Padley S. Imaging of congenital chest wall deformities. Br J Radiol 2016;89(1061):20150595 Restrepo CS, Martinez S, Lemos DF, et al. Imaging appearances of the sternum and sternoclavicular joints. Radiographics 2009;29(3):839–859Top Tips
Pectus excavatum is a common developmental anomaly of the anterior chest wall in which the sternum is caved in, creating a sunken appearance of the chest.
Most patients have a mild and clinically insignificant abnormality. However, severe cases can impair cardiac and respiratory function and cause chest and back pain.
The diagnosis of pectus excavatum is easily made on frontal and lateral chest radiographs. The right heart border is obscured on the frontal view, whereas the lateral view confirms the pectus deformity and excludes a consolidation.
Essentials 2
Case
A 19-year-old man with recurrent pneumonia and hemoptysis.

Questions
1. What is the MOST likely diagnosis?
A. Pulmonary sequestration
B. Lung abscess
C. Hilar lymphadenopathy
D. Congenital pulmonary airway malformation
E. Endobronchial tumor
2. Regarding typical course of this diagnosis, which ONE of the following is correct?
A. Carcinoid typically demonstrates poor contrast enhancement on CT.
B. Carcinoid typically demonstrates intense fluorodeoxyglucose (FDG) update on positron emission tomography/CT.
C. Calcification is seen in approximately 70% of pulmonary carcinoids.
D. A total of 80% of patients with carcinoid tumors are asymptomatic.
E. Pulmonary carcinoid arises from Kulchitsky cells in the bronchial epithelium.
3. Regarding pulmonary neuroendocrine tumors, which ONE of the following is correct?
A. Small cell lung carcinoma is the most common neuroendocrine lung neoplasm.
B. Neuroendocrine proliferations such as diffuse idiopathic neuroendocrine cell hyperplasia (DIPNECH) present as large masses.
C. Large cell neuroendocrine carcinoma (LCNEC) typically presents as a central endobronchial pulmonary mass.
D. Cushing syndrome is reported in approximately 25% of patients with pulmonary carcinoid.
E. Carcinoid syndrome is reported in approximately 25% of patients with pulmonary carcinoid.
Answers and Explanations
Question 1
E. Correct! This is a pulmonary carcinoid tumor. An enhancing endobronchial lesion typical of a vascular endobronchial pulmonary carcinoid is demonstrated.
Other choices and discussion
A. Pulmonary sequestration refers to the aberrant formation of segmental lung tissue that has no connection to the bronchial tree or pulmonary arteries. Sequestration preferentially affects the lower lobes. A total of 60% of intralobar sequestrations affect the left lower lobe, and 40% of intralobar sequestrations affect the right lower lobe. This entity may present in late childhood or adolescence with recurrent pulmonary infections. Cross-sectional imaging frequently demonstrates the arterial supply originating from the descending aorta and coursing into the lesion (although that is not shown in this case).
B. The chest computed tomography (CT) images demonstrate an enhancing left perihilar endobronchial lesion (note the curvilinear air density posteriorly suggesting an endobronchial location). The low attenuation material within the distal collapsed left lower lobe parenchyma represents accumulated endobronchial secretions. This does not have the appearance of an abscess.
C. The enhancing left endobronchial lesion is suggestive of a vascular tumor, rather than typical hilar lymphadenopathy.
D. CPAM is a multicystic mass comprised of segmental lung tissue with abnormal bronchial proliferation. Five subtypes are currently classified. Type I and II CPAMs demonstrate a multicystic (air-filled) lesion, but in type III, the lesion can present as a nonresolving consolidation. CPAM is typically diagnosed early in life and often in the perinatal period. It usually presents with tachypnea, cyanosis, and respiratory distress. However, rare cases are asymptomatic and undiagnosed until adulthood. There is no associated endobronchial mass in CPAM, as is shown in the test case.
Question 2
E. Correct! Kulchitsky cells are of neuroendocrine origin and are found in the epithelium of the digestive and respiratory tracts. Gastrointestinal tract carcinoids account for 90% of all carcinoids. The lung is the second most common location for a carcinoid tumor.
Other choices and discussion
A. Pulmonary carcinoid tumors typically demonstrate intense enhancement on CT. Postobstructive pneumonitis may be present.
B. FDG positron emission tomography is often negative because of the relatively low metabolism of a typical carcinoid tumor. FDG uptake may be seen in an atypical carcinoid, or one that has undergone dedifferentiation. If a pulmonary carcinoid is diagnosed, a better nuclear medicine test to assess for metastatic disease is an Octreotide scan (somatostatin analogue). This is often successfully used to diagnose and localize occult carcinoid tumors.
C. A total of 30% of pulmonary carcinoids demonstrate calcification on CT (only 5% of cases demonstrate calcification on plain film).
D. A total of 25% of patients with typical lung carcinoid tumors are asymptomatic. In symptomatic patients, the most common presentation is persistent cough, hemoptysis, and recurrent or obstructive pneumonitis. Rarely, paraneoplastic syndromes can be the initial symptoms of either typical or atypical pulmonary carcinoid tumors. Some of the endocrinopathies that can be produced by a pulmonary carcinoid tumor include carcinoid syndrome, hypercortisolism and Cushing syndrome, inappropriate secretion of antidiuretic hormone, increased pigmentation secondary to excess melanocyte-stimulating hormone, and ectopic insulin production resulting in hypoglycemia. Atypical carcinoid sometimes initially presents with metastatic disease. Carcinoid syndrome is most likely to occur when there is metastatic disease to the liver.
Question 3
A. Correct! Small cell lung carcinoma is the most common neuroendocrine lung neoplasm, representing 15 to 20% of invasive lung malignancies. It is also one of the most aggressive cell types of primary lung cancer.
Other choices and discussion
B. DIPNECH is one of the manifestations of neuroendocrine proliferation in the lungs. DIPNECH is seen as multiple pulmonary micronodules, with or without associated mosaic attenuation or air trapping on high-resolution chest CT. Typical symptomatic patients with DIPNECH are females in their fifth to seventh decade with a history of cough and dyspnea. About half of patients with DIPNECH are asymptomatic and diagnosed incidentally on CT.
C. LCNEC typically manifests as a large, peripheral pulmonary mass ranging from 2 to 10 cm. It is a high-grade malignancy with neuroendocrine histologic features. Most patients are males in their fifth or sixth decade with a history of heavy smoking.
D. Pulmonary carcinoid rarely presents with paraneoplastic syndromes. Cushing syndrome is reported in only 2% of bronchial carcinoids. When present, it is characterized by an acute onset high concentration of adrenocorticotropic hormone and hypokalemia.
E. Although carcinoid syndrome is reported in 9% of patients with gastrointestinal carcinoids, it is seen at presentation in only 0.7% of patients with pulmonary carcinoids.
Top Tips
Carcinoid is a low-grade malignant neuroendocrine neoplasm with metastatic potential.
Consider pulmonary carcinoid tumor in symptomatic young or middle-aged patients with a well-defined central enhancing mass and an endoluminal component.
Four major types of neuroendocrine neoplasms are recognized, and these are grouped into three histologic grades. Typical carcinoid is the low-grade malignant neoplasm, atypical carcinoid is the intermediate-grade neoplasm, and LCNEC and small cell lung carcinoma are the high-grade neoplasms.
Essentials 3
Case
A 26-year-old man with an incidental finding on chest X-ray (CXR).

Questions
1. What is the MOST likely diagnosis?
A. Fibrosing mediastinitis
B. Pulmonary sequestration
C. Swyer-James syndrome
D. Hypogenetic lung syndrome
E. Meandering pulmonary vein
2. Which of the following are CORRECT concerning pulmonary venolobar syndrome? (Select ALL that apply.)
A. Defined as the partial or total anomalous pulmonary venous return of the right lung to the IVC just above or below the diaphragm
B. Also called Luftsichel syndrome
C. Associated abnormalities include abnormal right lung lobation and right lung hypoplasia
D. Scimitar vein is seen in 50% of cases
E. Majority are right sided
3. Which ONE of the following is correct?
A. Right PAPVR is associated with high sinus venosus atrial septal defect.
B. Left PAPVR is associated with high sinus venosus atrial septal defect.
C. Scimitar syndrome is a type of total anomalous venous drainage.
D. All cases of scimitar syndrome need surgical correction.
E. Meandering pulmonary vein is more common on the left side.
Answers and Explanations
Question 1
D. Correct! Hypogenetic lung syndrome (aka pulmonary venolobar syndrome or the scimitar syndrome) is a rare congenital disorder that consists of anomalous pulmonary venous drainage of the right lung to the inferior vena cava (IVC; giving rise to the scimitar sign), anomalous systemic arterial supply of the right lower lobe from either the thoracic or abdominal aorta, hypoplasia of the right lung, and resultant cardiac dextroposition and right pulmonary artery hypoplasia.
The curved vertical vein, representing the anomalous venous drainage, is seen paralleling the right heart border and directed toward the IVC, right atrium, or portal vein. CXR findings are that of a small lung with ipsilateral mediastinal shift. In one-third of cases, the anomalous draining vein may be seen as a tubular structure paralleling the right heart border in the shape of a Turkish sword (“scimitar”). There is associated congenital heart disease in 25% of cases.
Other choices and discussion
A. Fibrosing mediastinitis refers to a focal hilar or mediastinal mass that narrows the nearby airways or vessels. Calcification of the mass is common (60 to 90%). There is no mediastinal or hilar mass seen in the test case.
B. Pulmonary sequestration represents nonfunctioning lung tissue that is separated from normal lung and receives its blood supply from a systemic artery that lacks normal communication with the bronchi. On CXR, there is a persistent left-sided (65%) paraspinal mass. There is often a clinical history of recurrent pneumonia. The lung may contain solid, fluid, and cystic components (i.e., some have an air-fluid level). The identification of the systemic artery feeding the abnormal lung on computed tomography or magnetic resonance imaging is diagnostic. These findings are not present in the test case.
C. Swyer-James syndrome is characterized on radiography by a unilateral small lung with hyperlucency and air trapping, but with normal pulmonary venous anatomy. There is no vertical vein association with Swyer-James syndrome. This condition typically follows a viral respiratory infection such as adenoviruses or Mycoplasma pneumoniae in infancy or childhood.
E. With a meandering pulmonary vein, the scimitar sign is present in the right lung and the anomalous right pulmonary vein drains normally into the left atrium. This may therefore mimic a scimitar syndrome on CXR. However, there is no vascular shunt, and no treatment is required. For this reason, it is important to differentiate this condition from scimitar syndrome. Multidetector computed tomography allows clear depiction of the vascular connections and associated anatomy, and has superseded invasive pulmonary angiography and cardiac catheterization as the investigation of choice for differentiating meandering pulmonary vein from scimitar syndrome.
Question 2
A. Correct! Pulmonary venolobar syndrome is defined as the partial or total anomalous pulmonary venous return of the right lung to the IVC just above or below the diaphragm.
C. Correct! It is associated with abnormal right lung lobation and right lung hypoplasia in nearly all cases.
D. Correct! It has a scimitar (vertical) vein in 50% of patients (70% of pediatric/adult and 10% of infantile).
E. Correct! The majority are right sided.
Other choice and discussion
B. Pulmonary venolobar syndrome is called the “scimitar syndrome,” not the “Luftsichel syndrome.” The curved vertical vein paralleling the right heart border directed toward the midline is shaped like a “scimitar” (i.e., a Turkish sword).
Question 3
A. Correct! Because this type of atrial septal defect is clinically silent, the associated PAPVR may be the clue leading to the diagnosis of an atrial septal defect.
Other choices and discussion
B. This is incorrect.
C. Scimitar syndrome is a type of partial anomalous venous drainage with an anomalous pulmonary vein that drains into the IVC, the portal vein, or the hepatic veins below the diaphragm, and is associated with right pulmonary hypoplasia.
D. Most frequently, patients with scimitar syndrome are asymptomatic in the absence of associated abnormalities. Surgical correction is recommended for symptomatic patients or asymptomatic patients with a pulmonary to systemic blood flow exceeding 1.5 to 2 (because of their higher likelihood of progression to pulmonary hypertension and right ventricular failure).
E. Meandering pulmonary vein is more common on the right, is not associated with a shunt, and does not require further invasive investigation or management.
Top Tips
Scimitar syndrome, also called hypogenetic lung syndrome or congenital pulmonary venolobar syndrome, is a congenital hypoplasia of the right lung and anomalous pulmonary venous drainage, most commonly draining to the IVC.
The vertical vein is a gently curved vein in the right lung directed toward the right costovertebral angle. This vein enlarges as it descends toward the diaphragm. The anomalous vein is shaped like a Turkish sword, hence the name scimitar sign.
The majority are right sided.
Essentials 4
Case

Questions
1. Which ONE of the following is the MOST likely diagnosis?
A. Pulmonary Langerhans cell histiocytosis
B. Lymphangioleiomyomatosis
C. Centrilobular emphysema
D. Cystic fibrosis
E. Tuberous sclerosis
2. Regarding the diagnosis in the test case, which of the following are correct? (Select ALL that apply.)
A. The classic triad includes seizures, mental retardation, and adenoma sebaceum.
B. There are no associated imaging findings in the brain.
C. There is a significantly increased risk of renal cell carcinoma.
D. There is an association with pulmonary arterial hypertension, meconium ileus, pancreatic insufficiency, and cirrhosis.
3. All of the following are appropriate indications for high-resolution chest CT (HRCT) EXCEPT:
A. Diffuse lung disease
B. Solitary pulmonary nodule
C. Restrictive lung disease
D. Pulmonary hypertension
E. Obstructive lung disease
Answers and Explanations
Question 1
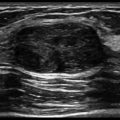
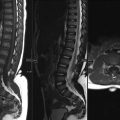
E. Correct! This is tuberous sclerosis (TS). The chest radiograph shows a diffuse reticular pattern. Closer inspection shows innumerable cystic air spaces. Computed tomography (CT) confirms a pattern of diffuse cystic lung disease, with cysts showing well-defined walls. In the abdomen, multiple angiomyolipomas (AMLs) are present in the right kidney. The left kidney is surgically absent.
Other choices and discussion
A. PLCH can be associated with a diffuse bilateral reticulonodular pattern with a predilection for the upper lungs. Later in the course of the disease, the irregular nodules can cavitate, giving the appearance of irregular cysts.
B. LAM can be associated with multiple thin-walled cysts throughout the lungs. Very small cysts can give the appearance of diffuse interstitial markings. Chylous pleural effusion are sometimes present. Associated pneumothorax can be seen with TS, PLCH, and LAM, but the left nephrectomy clips favor TS.
C. Visible walls make emphysema less likely. Lack of associated nodules also argues against emphysema.
D. Cystic fibrosis should show bronchiectasis (tram-tracking).
Question 2
A. Correct! The classic triad of TS includes seizures, mental retardation, and adenoma sebaceum. Less than half of the patients present with the complete triad.
Other choices and discussion
B. Multiple brain imaging findings may be present with TS. These include cortical/subcortical tubers, subependymal hamartomas, subependymal astrocytomas, and various white matter abnormalities.
C. The incidence of renal cell carcinoma in patients with TS is similar to that of the general population, but patients with TS tend to develop them at an earlier age. Angiomyolipoma is the renal mass classically associated with TS and may be multiple, as is demonstrated in the test case. AMLs often occur with aneurysms, which can sometimes be seen with imaging.
D. Pulmonary arterial hypertension, meconium ileus, pancreatic insufficiency and cirrhosis are associated with cystic fibrosis.
Question 3
B. Correct! Solitary pulmonary nodule is not typically an appropriate indication for HRCT.
Referring providers often misconstrue the high-resolution moniker as an indicator of the best lung evaluation (aka HDTV or 4K TV!). In truth, most centers perform HRCT as a sampling of the lung parenchyma with “noncontiguous” series, primarily to assess for patterns of diffuse lung disease, airway disease, or vascular disease. The noncontiguous technique, also referred to as “axial” or “sequential” imaging, is generally used to limit radiation. Thin collimation in HRCT requires more radiation on a per-slice basis to mitigate the extra image noise. Typi cal HRCTs include sampling of the lungs with full inspiration at 1-mm slice thickness at 10- to 20-mm intervals (aka 1 × 10 mm), rendering them inappropriate for initial characterization or follow up of solitary pulmonary nodules. Furthermore, typical HRCT protocols also include separate prone and expiratory imaging, adding additional radiation. These are necessary to assess for early subpleural fibrosis or air-trapping.
Initial workup of solitary pulmonary nodules should include an attempt to characterize three different features of the nodule: size, consistency (i.e., cavitation, calcification, or fat), and margins. Noncontrast standard protocol CT with 2.5- to 5-mm contiguous intervals is preferable (aka 2.5 × 2.5 mm), with contrast added for additional characterization if needed or for mediastinal assessment.
Other choices and discussion
A. HRCT is well suited for characterization of diffuse lung disease, as in the test case. HRCT can identify the predominant pattern and distribution of cystic, interstitial, and fibrotic lung disease. When paired with appropriate clinical inputs, useful differential diagnoses can be generated for guiding further investigations such as medical therapy, biochemical assays (autoimmune workup), or biopsy.
C. When pulmonary function testing indicates restriction or decreased lung volumes, the primary consideration is fibrotic lung disease. Key indicators of fibrotic lung disease on HRCT are honeycombing, traction bronchiectasis, architectural distortion, and decreased lung volume.
D. The majority of pulmonary hypertension is attributable to primary pulmonary arterial hypertension. Two important categories of secondary pulmonary hypertension are lung disease and vascular disease.
E. HRCT can be helpful in detecting both small and large airway obstruction. Small airway disease is typically manifest as air-trapping on expiratory imaging. Large airway disease can be manifest as bronchial wall thickening or large airway collapse involving the trachea or main bronchi on expiratory imaging.
Top Tips
Ground glass attenuation on HRCT often suggests an active and potentially reversible process.
Pulmonary hypertension is likely in patients older than 50 years of age if the ratio of the diameter of the main pulmonary artery to the ascending aorta (at the same level) is > 1.
Typical findings of cystic fibrosis in the lungs include mucous plugging, bronchiectasis, recurrent atelectasis and pneumonitis, and air trapping.
Essentials 5
Case
A 42-year-old man undergoes cross-sectional imaging following discovery of an incidental mass on chest X-ray.

Questions
1. What is the MOST likely diagnosis?
A. Pericardial cyst
B. Thymic cyst
C. Castleman disease
D. Bronchogenic cyst
E. Intrathoracic pancreatic pseudocyst
2. What is the MOST common location for this lesion?
A. Subcarinal region
B. Paratracheal region
C. Retrocardiac
D. Intrapulmonary
E. Pericardium
3. Which are the following is NOT a recognized complication of this lesion?
A. Fistula
B. Hemorrhage
C. Rhabdomyosarcoma
D. Abscess
E. Lymphoma
Answers and Explanations
Question 1
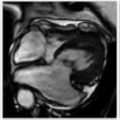
D. Correct! This is a bronchogenic cyst. The postcontrast computed tomography (CT) demonstrates a soft tissue density subcarinal mass. It demonstrates iso- to mildly hyperintense signal on T2-weighted magnetic resonance imaging (MRI), but it is lower signal intensity than cerebrospinal fluid and is hyperintense on precontrast T1. These imaging features are characteristic of a bronchogenic cyst, a congenital malformation of the bronchial tree. They are the most common type of foregut duplication cyst, accounting for approximately 50% of congenital mediastinal cysts. Bronchogenic cysts can cause symptoms from local compression, but are most often asymptomatic and discovered incidentally. On CT, they may be fluid or soft tissue density, depending on the presence of hemorrhage or proteinaceous contents. This proteinaceous content can cause them to appear iso- to mildly hyperintense signal on T1 MRI, and iso- to mildly hyperintense signal on T2 MRI.
Other choices and discussion
A. Pericardial cysts are typically located at the cardiophrenic angles, most commonly on the right, and are low attenuation on CT.
B. Thymic cysts typically occur in the anterior mediastinum. Congenital thymic cysts tend to be unilocular, with well-defined and frequently imperceptible walls. Multilocular thymic cysts are usually acquired secondary to hemorrhage, infection, or underlying malignancy. On MRI, thymic cysts are typically low signal on T1, high signal on T2, and have no enhancement on postgadolinium T1 imaging.
C. Castleman disease (angiofollicular lymph node hyperplasia or giant lymph node hyperplasia) is characterized by hypervascular lymphoid hyperplasia. This is a B-cell lymphoproliferative condition that commonly presents as a solitary mediastinal mass. It typically contains arborizing calcification on CT and is a solid mass with iso- to low signal intensity on T2-weighted MRI. Multicentric Castleman disease is a rare systemic disease with diffuse lymphadenopathy, anemia, and splenomegaly, and usually occurs in patients with human immunodeficiency virus.
E. Intrathoracic pancreatic pseudocysts are retroperitoneal cystic lesions that extend from the abdomen into the thorax through the aortic or esophageal hiatus. They originate from the pancreas and occur as a complication of pancreatitis.
Question 2
A. Correct! The mediastinum is the most common location for bronchogenic cysts, accounting for 65 to 90% cases, with the subcarinal location accounting for approximately 50% of total cases.
Other choices and discussion
B. Paratracheal location, most commonly on the right, accounts for approximately 20% cases.
C. Retrocardiac is an uncommon location, accounting for <10% of cases.
D. Intrapulmonary is an uncommon location; when present in an intrapulmonary location, they are typically perihilar and found in the lower lobes.
E. Pericardium is an uncommon location. The most common cystic lesion in the pericardium is a pericardial cyst.
Question 3
E. Correct! Lymphomatous transformation is a recognized complication of Castleman disease, but is not described in bronchogenic cysts.
Other choices and discussion
A. Fistula formation with the bronchial tree is a recognized complication of bronchogenic cysts. Instrumentation can lead to fistula formation, and this manifests as an air-fluid level in the cyst.
B. Intralesional hemorrhage is a common complication. It can occur spontaneously or secondary to intervention, manifesting on CT as layered high density material within the cyst.
C. Malignancy transformation is a rare (approximately 0.7%) complication, with reported tumors including rhabdomyosarcoma, leiomyosarcoma, and adenocarcinoma. This manifests on imaging as a new and enhancing solid component within the cyst.
D. Abscess complicates approximately 20% of bronchogenic cysts, usually occurring secondary to fistula formation with the tracheobronchial tree.
Suggested Readings
Berrocal T, Madrid C, Novo S, Gutiérrez J, Arjonilla A, Gómez-León N. Congenital anomalies of the tracheobronchial tree, lung, and mediastinum: embryology, radiology, and pathology. Radiographics 2004;24(1) Ko S-F, Hsieh M-J, Ng S-H, Lin J-W, Wan Y-L, Lee T-Y, et al. Imaging spectrum of Castleman’s disease. Am J Roentgenol 2004;3:769–775Top Tips
Bronchogenic cysts are the most common foregut duplication cyst and are usually found in the subcarinal, paratracheal, or perihilar regions.
On CT, they may be fluid or soft tissue density, depending on the proteinaceous content. They are T2 iso- to mildly hyperintense and do not enhance. Postcontrast subtraction images maybe helpful in lesions with intrinsic precontrast T1 hyperintensity (due to hemorrhage or protein) and also to exclude an enhancing soft tissue component.
Infection is the most common complication, usually occurring secondary to instrumentation of the tracheobronchial tree leading to fistula formation.
Essentials 6
Case
A 53-year-old man presents with abdominal distention.

Questions
1. What is the MOST common clinical presentation of bronchial atresia?
A. Asymptomatic patient
B. Focal wheeze on auscultation
C. Hemoptysis
D. Shortness of breath
E. Recurrent pneumonia
2. What is the MOST common presentation of this diagnosis on chest X-ray?
A. Hyperinflated lobe
B. Perihilar nodule
C. Bronchiectasis
D. Tubular/branching opacity
3. Where is the MOST common location for bronchial atresia?
A. Left upper lobe
B. Right upper lobe
C. Right middle lobe
D. Left lower lobe
Answers and Explanations
Question 1
A. Correct! Most patients with bronchial atresia are asymptomatic.
Other choices and discussion
This abnormality is usually an incidental finding on chest radiography. However, some patients may present with recurrent pneumonia. Focal wheeze on auscultation, hemoptysis, and shortness of breath are not commonly seen with bronchial atresia.
Question 2
A. Correct! A hyperinflated lobe is the most common radiographic appearance of bronchial atresia.
Other choices and discussion
Typically, chest radiographs of patients with bronchial atresia show an area of lobar hyperlucency (90%) and a hilar nodule or mass (80%). Mucoid-impacted airway may mimic a solitary pulmonary nodule. A hyperlucent lobe may be mistaken for congenital lobar emphysema, obstructing foreign body or, less likely, a Westermark sign (oligemia secondary to pulmonary embolism).
Question 3
A. Correct! The left upper lobe is the most common location for bronchial atresia.
Other choices and discussion
Bronchial atresia is a congenital abnormality thought to arise from a vascular insult in utero, after the fifteenth week of gestation. The result is a short segment obliteration of a lobar segmental or subsegmental bronchus near its origin. It most commonly involves the apical posterior segment of the left upper lobe.
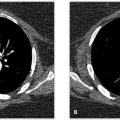
As is seen in this case, computed tomography (CT) imaging typically shows an area of pulmonary hyperlucency secondary to hyperinflation via collateral air drift (pores of Kohn and canals of Lambert) and decreased vascularity (oligemia). The adjacent lung is compressed and displaced. The focal rounded low density lesion represents the mucoid impacted dilated bronchus just distal to the bronchial obliteration. Another common radiographic appearance is tubular and branching densities, representing mucoid impacted airways, distal to the obliterated bronchus. CT is the most sensitive imaging technique for confirmation of the diagnosis.
It is important to make the correct diagnosis, as the main differential diagnosis for bronchial atresia includes endobronchial tumor and foreign body, and bronchoscopy is indicated for those entities. Clinical history that would increase suspicion for foreign body includes aspiration episode and traumatic intubation/recent dental work (i.e., broken tooth). Thin collimation CT is helpful to identify a possible foreign body and to measure the density of the obstructing lesion. A low-density focus (Hounsfield unit <25) is consistent with mucoid impaction if the density is tubular or branching in morphology.
Other less common diagnostic considerations for bronchial atresia include congenital lobar emphysema associated with a patent bronchus, allergic bronchopulmonary aspergillosis, pulmonary varix, arterial venous malformation, and postinfectious bronchial stricture secondary to Mycobacterium tuberculosis. Contrast-enhanced CT can better diagnose vascular abnormalities such as pulmonary varix and arterial venous malformation.
Suggested Readings
Dillman JR, Yarram SG, Hernandez RJ. Imaging of pulmonary venous developmental anomalies. Am J Roentgenol 2009;192(5):1272–1285 Kinsella D, Sissons G, Williams MP. The radiological imaging of bronchial atresia. Br J Radiol 1992;65(776):681–685 Schuster SR, Harris GB, Williams A, Kirkpatrick J, Reid L. Bronchial atresia: a recognizable entity in the pediatric age group. J Pediatr Surg 1978;13(6D):682–689Top Tips
Bronchial atresia is usually asymptomatic, but may present with recurrent pneumonia.
The main differential diagnosis for bronchial atresia includes endobronchial tumor and foreign body.
Less common diagnostic considerations for bronchial atresia include congenital lobar emphysema associated with a patent bronchus, allergic bronchopulmonary aspergillosis, pulmonary varix, arterial venous malformation, and postinfectious bronchial stricture secondary to Mycobacterium tuberculosis.
Essentials 7
Case
A 69-year-old man status post attempted transesophageal echocardiogram; preoperative for atrial flutter ablation.

Questions
1. What is the MOST likely diagnosis?
A. Mediastinitis
B. Esophageal tear
C. Empyema necessitans
D. Bronchial rupture
2. Given the location of the defect, what is the MOST common cause?
A. Boerhaave
B. Iatrogenic
C. Caustic ingestion
D. Perforated ulcer
3. What complication is visualized on the above images?
A. Esophageal pleural fistula
B. Esophageal bronchial fistula
C. Empyema
D. Mediastinitis
Answers and Explanations
Question 1
B. Correct! This is an esophageal tear. Extravasation of contrast on the esophagram is diagnostic.
If an esophageal tear is suspected, the next most appropriate imaging modality is an esophagram with water-soluble contrast. Indirect signs of esophageal perforation on chest radiography include subcutaneous emphysema, widened mediastinum, and left pleural effusion.
The other choices are incorrect.
Question 2
B. Correct! Iatrogenic causes account for the majority of esophageal perforations (56% of cases).
Other choices and discussion
The term Boerhaave syndrome is reserved for esophageal perforations that occur secondary to vomiting (10% of cases). Patients typically present with chest pain that radiates to the back or left shoulder, causing physicians to confuse an esophageal perforation with a myocardial infarction.
While iatrogenic esophageal perforations can occur anywhere, in most cases of Boerhaave syndrome, the tear occurs at the left posterior and lateral aspect of the distal esophagus. The classical presentation is named Mackler triad, which includes chest pain, vomiting, and subcutaneous emphysema.
Other etiologies of perforation include foreign bodies (chicken and fish bones), caustic ingestion, pill esophagitis, Barrett esophagus, and iatrogenic following dilatation for strictures. Of note, a series of esophageal perforations has been reported in the literature as the sequelae of ablation for atrial fibrillation. Ablations occur near the ostia of the pulmonary veins within the left atrium, and the adjacent esophagus traveling along the posterior aspect of the left atrium is sometimes injured.
Question 3
D. Correct! Mediastinitis is demonstrated.
Dreaded complications of esophageal perforation are mediastinitis and sepsis, which can result in high morbidity and mortality. Other complications include abscess, esophageal/bronchial/pleural fistulas, and empyema.
Treatment consists of immediate antibiotic therapy (to prevent mediastinitis and sepsis) and surgical repair of the perforation. In this case, the patient was taken to the operating room to drain the mediastinal collection and to repair the esophageal tear.
Suggested Readings
De Lutio di Castelguidone E, Pinto A, Merola S, Stavolo C, Romano L. Role of spiral and multislice computed tomography in the evaluation of traumatic and spontaneous oesophageal perforation. Our experience. Radiol Med 2005;109(3):252–259
Lee S, Mergo PJ, Ros PR. The leaking esophagus: CT patterns of esophageal rupture, perforation, and fistulization. Crit Rev Diagn Imaging 1996;37(6):461–490
Tocino I, Armstrong J. Trauma to the lung. In: Taveras J, ed. Radiology. Philadelphia, PA: Lippincott-Raven; 1996: 1–8
Top Tips
Fish and chicken bones are best imaged with computed tomography. Fish bones contain less calcium and are less opaque than chicken bones. If plain films are negative and there is a high index of suspicion, either contrast esophagram or computed tomography is indicated.
Other causes of pneumomediastinum include tracheal injury, excessive coughing, barotrauma (intubated patient with increasing positive end expiratory pressure), rapid rises in altitude (scuba diving), and the use of recreational drugs such as crack cocaine.
Esophageal perforations have been reported as the sequelae of ablation for atrial fibrillation.
Essentials 8
Case
A 53-year-old woman with 20 pack-year smoking history presents with right shoulder pain.

Questions
1. What radiographic abnormality is demonstrated?
A. Neurogenic tumor
B. Mycobacterial infection (tuberculosis)
C. Postradiation fibrosis
D. Lung carcinoma
2. What is the MOST common clinical presentation for this disease entity?
A. Hemoptysis
B. Shoulder pain
C. Horner syndrome
D. Pleuritic chest pain
3. What is the most common histologic type of this apical abnormality?
A. Squamous cell
B. Adenocarcinoma
C. Neuroendocrine
D. Sarcomatoid
Answers and Explanations
Question 1
D. Correct! This is most likely lung carcinoma.
The differential diagnosis of apical cap/mass includes extrapleural fat, inflammatory disease (tuberculosis), neurogenic tumor, mesothelioma, and radiation fibrosis. Bony destruction of the right apical first rib and a smoking history favor the diagnosis of Pancoast tumor. In this case, both the brachial plexus and subclavian vessels were encased by tumor.
Magnetic resonance imaging with its superior soft tissue contrast permits better evaluation of the brachial plexus, subclavian vessels, and possible chest wall involvement. Positron emission tomography/computed tomography allows assessment of nodal and distant metastasis and is helpful for staging.
The other choices are incorrect.
Question 2
B. Correct! Shoulder pain is the most common clinical presentation. Pancoast (or superior sulcus) tumor is a smoking-related cancer of lung origin. Clinically, patients often present with shoulder pain radiating down the arm due to brachial plexus involvement. (This patient presented with weight loss and shoulder pain.)
Less commonly (25%), patients present with Horner syndrome (ptosis, miosis, and hemifacial anhidrosis) when the stellate plexus is involved. By definition, Pancoast tumors involve the parietal pleura and include periosteal/bony involvement of the upper ribs or apical vertebral bodies. With newer surgical approaches and combined use of chemotherapy and radiation therapy, these tumors may be resectable even with vertebral body or neural foramen involvement.
Question 3
A. Correct! Although Pancoast tumors may be any histologic type, squamous cell is most common.
The other choices are incorrect.
Note that the “pack-year” is a unit for measuring the amount a person has smoked over a long period of time.
Number of pack-years = (number of cigarettes smoked per day/20) × number of years smoked. (One pack has 20 cigarettes.)
For example, if a patient smoked 15 cigarettes per day for 20 years, that amounts to 15 pack-years.
Suggested Readings
Heelan RT, Demas BE, Caravelli JF, et al. Superior sulcus tumors: CT and MR imaging. Radiology 1989;170(3 Pt 1):637–641 Pancoast HK. Superior pulmonary sulcus tumor: tumor characterized by pain, Horner’s syndrome, destruction of bone and atrophy of hand muscles. JAMA 1932;99:1391–1396 Webb WR, Gatsonis C, Zerhouni EA, et al. CT and MR imaging in staging non-small cell bronchogenic carcinoma: report of the Radiologic Diagnostic Oncology Group. Radiology 1991;178(3):705–713Top Tips
Number of pack-years = (number of cigarettes smoked per day/20) × number of years smoked.
Musculoskeletal radiologists should keep Pancoast tumor in mind when reviewing dedicated shoulder radiographs for shoulder pain.
Asymmetric pleural thickening has many causes. Benign causes include postinfectious (prior tuberculosis), abscess, radiation fibrosis, idiopathic, and hematoma (posttrauma, aortic injury). Malignant causes include Pancoast tumor, lymphoma, and mesothelioma.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


