SECTION XII US/REPRODUCTIVE/ENDOCRINOLOGY IMAGING
Essentials 1
Case
A patient has intense tenderness when the sonographer presses the transducer probe over the right upper quadrant of the abdomen. Grayscale longitudinal image of the right upper quadrant (a) and longitudinal image of the right upper quadrant with Doppler (b) are shown.

Questions
1. Which ONE of the following is the most likely diagnosis?
A. Acute acalculous cholecystitis
B. Acute calculous cholecystitis
C. Adenomyomatosis
D. Gallbladder carcinoma
E. Emphysematous cholecystitis
2. Which ONE of the following is the most sensitive sign for this condition?
A. Air within the gallbladder lumen
B. Sonographic Murphy sign
C. Presence of gallstones
D. Decreased vascular flow to the gallbladder wall on Doppler
E. Gallbladder distention
3. Which ONE of the following is a feature of emphysematous cholecystitis?
A. More common in women than men
B. Gallstones are present in 85% of cases
C. Gallstones are almost never present
D. Isolated condition not usually associated with systemic metabolic disorders
E. Surgical emergency due to risk of perforation
Answers and Explanations
Question 1
B. Correct! This is acute calculous cholecystitis. This has the classic appearance of an obstructing stone in the gallbladder neck, with wall thickening, and wall hyperemia on Doppler. (As noted in the history, there was a reported positive sonographic Murphy sign as well.)
Other choices and discussion
A. Gallstones are present, excluding acalculous cholecystitis. Acute inflammation of the gallbladder in the absence of stones is termed acalculous cholecystitis.
C. The classic “comet-tail” artifact of adenomyomatosis is not present in this case.
D. No mass lesion or mass-like wall thickening is present to suggest neoplasm.
E. No air or “dirty shadowing” is present to suggest emphysematous cholecystitis.
Question 2
B. Correct! The sonographic Murphy sign is the most sensitive sign for this diagnosis. A sonographic Murphy sign refers to pain from transducer palpation over the gallbladder with inspiration. A sonographic Murphy sign is associated with 90% of cases of acute cholecystitis. Typically, the gallbladder is visualized, and the patient is instructed to take a deep breath while the sonographer increases transducer pressure.
Other choices and discussion
A. Air within the gallbladder lumen is a very uncommon finding. In the setting of emphysematous cholecystitis, air is present within the wall of the gallbladder.
C. The presence of gallstones (cholelithiasis) is common, but not the most sensitive finding. In addition, gallstones are often seen in the absence of acute inflammation. Gallstones may be clinically asymptomatic or result in intermittent biliary colic.
D. Vascular flow is typically increased in the setting of acute cholecystitis, although this is not the most sensitive finding. Pronounced flow in the cystic artery is occasionally seen with Doppler.
E. Gallbladder distention commonly occurs with fasting in normal patients.
Question 3
E. Correct! Emphysematous cholecystitis is a surgical emergency. Emphysematous cholecystitis refers to acute inflammation of the gallbladder due to gas-forming bacteria. It carries an increased risk of gallbladder perforation, peritonitis, sepsis, and death. Therefore, emergent cholecystectomy is indicated.
Other choices and discussion
A. Emphysematous cholecystitis is seven times more common in males than in females.
B. Up to half of the patients with emphysematous cholecystitis do not have gallstones.
C. Up to half of the patients with emphysematous cholecystitis do not have gallstones.
D. The prevalence of emphysematous cholecystitis is increased in patients with metabolic disorders. Up to one-half of the patients with emphysematous cholecystitis have diabetes mellitus.
Suggested Readings
Cooperberg PL, Burhenne HJ. Real-time ultrasonography. Diagnostic technique of choice in calculous gallbladder disease. N Engl J Med 1980;302:1277–1279 Konno K, Ishida H, Naganuma H, et al. Emphysematous cholecystitis: sonographic findings. Abdom Imaging 2002;27:191–195 Singer AJ, McCracken G, Henry MC, Thode HC Jr, Cabahug CJ. Correlation among clinical, laboratory, and hepatobiliary scanning findings in patients with suspected acute cholecystitis. Ann Emerg Med 1996;28:267–272Top Tips
The patient should fast for at least 4 hours prior to an ultrasound examination for possible acute cholecystitis. (The gallbladder should be distended during the ultrasound examination for optimal assessment.)
The hallmark of gallbladder carcinoma is a discrete immobile mass with vascular flow. Conversely, gallstones and sludge will move to the dependent portion of the gallbladder and are avascular vascularity. Use mobility and vascularity to differentiate these two entities.
Be careful when concluding that there is a positive sonographic Murphy sign. Many people use the term loosely to describe pain on transducer palpation anywhere in the right upper quadrant. A true positive sign refers to pain directly over the visualized gallbladder with transducer pressure and patient inspiration.
Essentials 2
Case
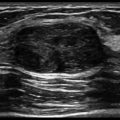
The patient is currently asymptomatic. Grayscale longitudinal image of the right upper quadrant (a) and grayscale longitudinal decubitus image of the right upper quadrant (b) are shown.

Questions
1. Which ONE of the following the most likely diagnosis?
A. Acute acalculous cholecystitis
B. Acute calculous cholecystitis
C. Adenomyomatosis
D. Gallbladder carcinoma
E. Emphysematous cholecystitis
2. What is the malignant potential of this condition?
A. No malignant potential
B. Premalignant condition that develops into gallbladder carcinoma in 20% of cases
C. If untreated, nearly always leads to cholangiocarcinoma
D. Questionable association with carcinoma, but incidentally found on nearly all specimens of resected gallbladder cancer
E. Associated with sarcomatous transformation
3. What is the etiology of this condition?
A. Small gallstones adherent to the gallbladder wall
B. Intramural gas within the gallbladder wall
C. Prominent Rokitansky-Aschoff sinuses
D. Intraluminal calculi
E. Inflammatory polyps
Answers and Explanations
Question 1
C. Correct! This is adenomyomatosis. Pictured is the classic “comet-tail” artifact, which occurs secondary to ultrasound wave reflections off cholesterol crystals within sinuses of the gallbladder wall.
Other choices and discussion
A. No sonographic signs are seen to suggest cholecystitis, such as gallbladder wall thickening or pericholecystic fluid. In addition, the patient is reportedly asymptomatic.
B. No gallstones are seen.
D. No mass lesion or mass-like wall thickening is seen.
E. Air would result in more pronounced shadowing in the gallbladder wall than is seen in the test case, and the patient would likely be symptomatic with emphysematous cholecystitis.
Question 2
A. Correct! Adenomyomatosis has no malignant potential. While adenomyomatosis has been identified in some resected gallbladder carcinoma specimens, no direct relationship between the two conditions has been definitively established.
Discussion
The other options are incorrect. Surgical treatment of isolated adenomyomatosis is not indicated in the absence of symptoms.
Question 3
C. Correct! The hallmark of adenomyomatosis is prominent epithelial sinuses (Rokitansky-Aschoff sinuses), which herniate into the gallbladder wall. Cholesterol crystals may deposit in these sinuses, giving a characteristic comet-tail artifact.
Other choices and discussion
A. This is not due to adherent gallstones.
B. This is not due to intramural gas. Intramural gas is seen in the setting of emphysematous cholecystitis and is a surgical emergency, due to the risk of gallbladder perforation. It does not progress to adenomyomatosis.
D. Patients with adenomyomatosis may also have cholecystitis. However, this condition does not lead to the formation of adenomyomatosis.
E. Inflammatory polyps are a less common form of gallbladder polyposis. They are usually associated with longstanding cholelithiasis.
Suggested Readings
Nishimura A, Shirai Y, Hatakeyama K. Segmental adenomyomatosis of the gallbladder predisposes to cholecystolithiasis. J Hepatobiliary Pancreat Surg 2004;11:342–347 Raghavendra BN, Subramanyam BR, Balthazar EJ. Sonography of adenomyomatosis of the gallbladder: radiologic-pathologic correlation. Radiology 1983;146:747–752Top Tips
Adenomyomatosis is commonly asymptomatic and can be an incidental finding on gallbladder ultrasound.
Adenomyomatosis should not be confused with “adenomyosis,” which is a condition affecting the uterine endometrium and myometrium. (Clue: adenomyomatosis has a “T” in it, and is located at the “top” of the abdomen.)
Cholecystectomy is often recommended for gallbladder polyps that are > 1 cm, increasing in size, or symptomatic.
Essentials 3
Case
Ultrasound of the right upper quadrant was obtained in a 20-year-old patient with intermittent abdominal pain. Grayscale longitudinal images of the liver with (a) and without (b) Doppler are shown.

Questions
1. Which ONE of the following is the most likely diagnosis?
A. Hemangioma
B. Fibrolamellar hepatocellular carcinoma
C. Abscess
D. Cirrhosis
E. Postbiopsy pseudoaneurysm
2. What is the MOST common presentation of this disorder?
A. Incidental finding on imaging
B. Acute intrahepatic hemorrhage
C. Elevated transaminases
D. Thrombocytopenia
E. Metastasis
3. Which ONE of the following is a common imaging characteristic of this disorder on ultrasound?
A. Size > 6 cm
B. Intense vascular flow on Doppler
C. Heterogeneous appearance with internal necrosis
D. Anechoic signal
E. Homogeneous hyperechoic mass
Answers and Explanations
Question 1
A. Correct! This is a hemangioma. Hepatic hemangiomas typically present as well-defined hyperechoic masses with no flow on Doppler. They are common incidental findings on imaging of the liver, with some studies reporting them in up to 20% of the population.
Other choices and discussion
B. Fibrolamellar hepatocellular carcinoma is a hepatic mass that typically presents in 20- to 40-year-olds. Although it is less aggressive than hepatocellular carcinoma, it does not produce symptoms until later in the disease, so it often presents as a large mass, unlike the test case.
C. Abscess would present as a complex fluid collection.
D. This patient does not have the nodular liver contour or heterogeneous echotexture seen in cirrhosis.
E. Pseudoaneurysm is a highly vascular lesion. It is usually the result of trauma or prior intervention.
Question 2
A. Correct! Cavernous hemangiomas are frequently found incidentally on ultrasound, computed tomography, and magnetic resonance imaging examinations. They are the most common benign liver lesion.
Other choices and discussion
B. While large hemangiomas (> 5 cm) can hemorrhage, most cavernous hemangiomas are smaller and do not bleed.
C. Most hemangiomas are asymptomatic and do not affect liver enzyme levels.
D. Consumptive coagulopathy can occur in the setting of Kasabach-Merritt syndrome in infants, but the vast majority of hemangiomas are asymptomatic.
E. This is a benign lesion, so it would not present with metastatic disease.
Question 3
E. Correct! A homogeneous hyperechoic mass is the most common sonographic appearance of a hepatic cavernous hemangioma.
Other choices and discussion
A. Giant and symptomatic hemangiomas can occur, although the majority of cavernous hemangiomas are small (< 5 cm).
B. While some hemangiomas can have flow, that flow is typically slow and may not be visualized on Doppler. In fact, most hemangiomas have no flow on Doppler.
C. Necrosis is not a typical feature of cavernous hemangiomas.
D. Hepatic hemangiomas can have a varied appearance on ultrasound, but most are hyperechoic.
Suggested Readings
McArdle CR. Ultrasonic appearances of a hepatic hemangioma. J Clin Ultrasound 1978;6:124 Mungovan JA, Cronan JJ, Vacarro J. Hepatic cavernous hemangiomas: lack of enlargement over time. Radiology 1994;191:111–113 Perkins AB, Imam K, Smith WJ, Cronan JJ. Color and power Doppler sonography of liver hemangiomas: a dream unfulfilled? J Clin Ultrasound 2000;28:159–165 Tait N, Richardson AJ, Muguti G, Little JM. Hepatic cavernous haemangioma: a 10 year review. Aust N Z J Surg 1992;62:521–524Top Tips
Computed tomographic (CT) features of hemangioma include peripheral, nodular, discontinuous enhancement. Areas of discontinuous enhancement will later fill in and become more homogeneous on delayed phases. Larger hemangiomas sometimes do not completely fill in centrally.
Some hemangiomas may show fast homogenous enhancement, termed “flash filling.” These are usually smaller.
A typical hemangioma matches the blood pool on all phases of contrast.
Essentials 4
Case
Transverse images of the liver with (a) and without (b) Doppler are shown.

Questions
1. Which ONE of the following is the most likely diagnosis?
A. Hepatocellular carcinoma
B. Acute hepatitis
C. Abscess
D. Hemangioma
E. Biliary obstruction
2. Which ONE of the following is NOT a predisposing factor for developing this disorder?
A. Hepatitis B
B. Hepatitis C
C. Hepatitis E
D. Alcohol abuse
E. Aflatoxins
3. Which ONE of the following is a characteristic of fibrolamellar hepatocellular carcinoma?
A. Found in elderly patients
B. Small tumor size
C. Multifocal distribution
D. Contains calcification
E. Associated decreased serum alpha-fetoprotein level
Answers and Explanations
Question 1
A. Correct! A large solid mass is present in the right lobe of the liver. Doppler demonstrates vascular flow within the lesion.
Other choices and discussion
B. Acute hepatitis can present as an enlarged liver with a somewhat hypoechoic hepatic parenchyma. The portal triads remain echogenic, giving the “starry sky” appearance.
C. Abscess presents as a complex fluid collection.
D. Hemangiomas typically present as well-defined hyperechoic masses with no flow on Doppler.
E. Biliary obstruction would cause biliary dilation, which is not seen in this case.
Question 2
C. Correct! Hepatitis E causes acute viral hepatitis and is commonly a co-infection with other viral types. However, it does not predispose to the development of hepatocellular carcinoma (HCC).
Discussion
The other options are incorrect—that is, they are all risk factors for developing HCC. This includes chronic hepatitis B and C, chronic alcohol use, and aflatoxins (fungal toxins used in grains).
Question 3
D. Correct! Fibrolamellar HCC commonly demonstrates internal calcification, which is a distinguishing feature.
Other choices and discussion
A. Fibrolamellar HCC typically presents in patients before the fourth decade of life, and it may occur in adolescents.
B. Fibrolamellar HCC typically presents as a large circumscribed mass lesion and has been reported at > 20 cm in size at the time of diagnosis.
C. Fibrolamellar HCC typically presents as a large solitary mass lesion and is rarely multifocal.
E. Alpha-fetoprotein levels are usually normal in patients with fibrolamellar HCC. Less than 10% of cases have increased levels.
Suggested Readings
El-Serag HB, Davila JA. Is fibrolamellar carcinoma different from hepatocellular carcinoma? A US population-based study. Hepatology 2004;39:798–803 El-Serag HB, Kanwal F. Epidemiology of hepatocellular carcinoma in the United States: where are we? Where do we go? Hepatology 2014;60:1767–1775 Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011;61:69–90 Kuniholm MH, Purcell RH, McQuillan GM, et al. Epidemiology of hepatitis E virus in the United States: results from the Third National Health and Nutrition Examination Survey, 1988-1994. J Infect Dis 2009;200:48–56Top Tips
Patients at high risk for developing HCC should be screened with imaging every 6 months.
Abnormal findings on ultrasound should prompt further workup with computed tomography and/or magnetic resonance imaging.
Fibrolamellar carcinoma is a rare form of HCC seen most commonly in young patients. It is less aggressive than typical HCC, although the stage at presentation is often advanced, as symptoms usually present late.
Essentials 5
Case
Grayscale transverse image of the left kidney (a) and longitudinal image of the left kidney with Doppler (b) are shown.

Questions
1. Which of the following is(are) in the differential diagnosis? Select ALL that apply.
A. Multicystic dysplastic kidney
B. Acquired renal cystic disease
C. Autosomal dominant polycystic kidney disease
D. Lithium nephrotoxicity
E. Renal lymphoma
2. Which ONE of the following is a feature of this condition?
A. Common cause of cystic renal disease in utero and in infancy
B. Usually progresses to fulminant renal failure
C. Multiple cysts communicate with one another and with the collecting system
D. Commonly bilateral
3. Which ONE of the following is included in the management of multicystic dysplastic kidney?
A. Screening the contralateral kidney for reversible abnormalities
B. Percutaneous nephrostomy
C. Retrograde ureteral stent placement
D. Biopsy at diagnosis to exclude superimposed neoplasm
E. Surgical resection of the affected kidney
Answers and Explanations
Question 1
A. Correct! Multicystic dysplastic kidney (MCDK) is characterized by multiple, large, noncommunicating cysts that distort the normal renal parenchyma.
B. Correct! Acquired renal cystic disease arises in patients who have undergone chronic dialysis therapy. It is characterized by multiple cysts of varying sizes. The intervening renal parenchyma is shrunken and echogenic.
C. Correct! Autosomal dominant polycystic kidney disease is characterized by numerous cysts. Patients may also have cystic involvement of the liver and pancreas.
Other choices and discussion
D. Lithium toxicity is a cause of cystic renal disease. However, the kidney develops microcysts, which are much smaller than the ones shown in the test case.
E. Renal lymphoma is an infiltrative process presenting as renal enlargement and solid masses that are usually hypoechoic. Cysts are not typical.
Question 2
A. Correct! MCDK is the most common cause of cystic renal disease early in life.
Other choices and discussion
B. Most cases are unilateral with preservation of contralateral renal function.
C. MCDK is characterized by multiple, noncommunicating cysts with a markedly distorted renal parenchyma. The cysts do not communicate with the collecting system, which differentiates this condition from ureteropelvic junction (UPJ) obstruction.
D. MCDK is commonly unilateral. If both kidneys are involved, it can be lethal.
E. Contralateral abnormalities, including vesicoureteral reflux and UPJ obstruction, have been reported in over 25% of patients with MCDK. These contralateral conditions require prompt diagnosis and correction to prevent the progression to renal failure.
Question 3
A. Correct! Screening of the contralateral kidney is indicated. Contralateral abnormalities, including vesicoureteral reflux and UPJ obstruction, have been reported in over 25% of patients with MCDK. These contralateral conditions may impair renal function, and cause hypertension.
Other choices and discussion
B. Because the affected kidney is nonfunctional, percutaneous nephrostomy is not indicated.
C. The collecting system of the nonfunctional kidney often cannot be visualized. Ureteral stent placement would not affect patient outcome.
D. MCDK is typically self-limiting. The cysts and the kidney tend to decrease in size with time.
E. Resection is rarely necessary, usually when when the kidney is massively enlarged.
Suggested Readings
Eckoldt F, Woderich R, Smith RD, Heling KS. Antenatal diagnostic aspects of unilateral multicystic kidney dysplasia—sensitivity, specificity, predictive values, differential diagnoses, associated malformations and consequences. Fetal Diagn Ther 2004;19:163–169 Onal B, Kogan BA. Natural history of patients with multicystic dysplastic kidney-what followup is needed? J Urol 2006;176:1607–1611 Stuck KJ, Koff SA, Silver TM. Ultrasonic features of multicystic dysplastic kidney: expanded diagnostic criteria. Radiology 1982;143:217–221Top Tips
In patients with MCDK, imaging of the contralateral kidney is necessary to screen for UPJ obstruction and reflux. These must be corrected in order to preserve renal function.
Real-time cine imaging is helpful in differentiating multiple noncommunicating cysts from hydronephrosis.
When evaluating for hydronephrosis, always check postvoid to make sure that it persists, and always use Doppler to exclude vessels that can mimic hydronephrosis.
Essentials 6
Case
History of recent endoscopic retrograde cholangiopancreatography to remove a retained distal bile duct stone after cholecystectomy. Grayscale transverse images of the liver are shown.

Questions
1. Which ONE of the following is the most likely diagnosis?
A. Acute uncomplicated cholecystitis
B. Cholangiocarcinoma
C. Pneumobilia
D. Hepatic granulomatous disease
E. Biliary polyps
2. Select ALL of the following conditions that may result in this disorder.
A. Emphysematous cholecystitis
B. Biliary-enteric fistula
C. Mesenteric ischemia
D. Sphincterotomy at the sphincter of Oddi
E. Acute cholangitis
3. Which ONE of the following is the recommended treatment for emphysematous cholecystitis?
A. Follow up ultrasound in 8 hours after confirming fasting status
B. Repeat ultrasound in 1 week
C. No follow up is necessary
D. Long-term therapy with broad-spectrum antibiotics
E. Emergent cholecystectomy
Answers and Explanations
Question 1
C. Correct! This is pneumobilia. Punctate echogenic foci within the biliary system are seen, consistent with air.
Other choices and discussion
A. Air would not be present within the biliary system in uncomplicated acute cholecystitis. This patient is status post cholecystectomy.
B. Cholangiocarcinoma would demonstrate biliary wall thickening and/or a mass lesion, not air.
D. Hepatic granulomatous disease would present as echogenic foci within the hepatic parenchyma, not within the biliary tree.
E. Polyps are discrete masses, not intraluminal mobile foci.
Question 2
A. Correct! With emphysematous cholecystitis, air collects in the gallbladder wall and may enter the biliary system. Emphysematous cholecystitis is a life-threatening condition and occurs more frequently in diabetics.
B. Correct! Biliary-enteric fistulae are commonly created surgically or can arise spontaneously in the setting of a gallstone ileus. Such fistulae allow air in the bowel to communicate with the biliary tree.
D. Correct! A sphincterotomy is sometimes performed during endoscopy to remove obstructing stones and to image the common bile duct. As a result, air may pass retrograde from the duodenum through the sphincter of Oddi and into the biliary tree.
E. Correct! Acute cholangitis classically presents with the Charcot triad: fever, jaundice, and right upper quadrant pain. Progression of this condition can sometimes lead to pneumobilia. Parasitic infections such as Clonorchis may be responsible. Ultrasound often demonstrates biliary sludge or air. Emergent treatment is necessary to decompress the biliary system.
Discussion
The other choice is incorrect. Mesenteric ischemia is a life-threatening condition seen with necrotic bowel. Air dissects from the necrotic bowel wall into the portal venous system, not the biliary tree. Portal venous gas usually has a more peripheral location on imaging than does biliary air, which is typically located centrally.
Question 3
E. Correct! Immediate surgical intervention is indicated for emphysematous cholecystitis.
The other choices are incorrect.
Suggested Readings
Bennett GL, Balthazar EJ. Ultrasound and CT evaluation of emergent gallbladder pathology. Radiol Clin N Am 2003;41:1203–1216 Sherman SC, Tran H. Pneumobilia: benign or life-threatening. J Emer Med 2006;30:147–153Top Tips
Biliary air presents as echogenic intraluminal foci within the biliary tree. Real-time imaging demonstrates that the air predominates centrally, mimicking the flow of bile.
Portal venous air occurs within the vessels and implies mesenteric ischemia, which can be life-threatening.
Portal venous air has a more peripheral distribution than does biliary air.
Essentials 7
Case
This patient presents for routine screening ultrasound of the abdomen. Grayscale longitudinal image of the right upper quadrant (a) and grayscale longitudinal image of the spleen (b) are shown.

Questions
1. Which ONE of the following is the most likely diagnosis?
A. Portal hypertension
B. Hepatocellular carcinoma
C. Acute hepatitis
D. Ascending cholangitis
E. Hepatic metastatic disease
2. What is the MOST common malignancy associated with cirrhosis?
A. Hepatocellular carcinoma
B. Fibrolamellar carcinoma
C. Angiosarcoma
D. Hepatic hemangioma
E. Focal nodular hyperplasia
3. Which ONE of the following is a feature of chronic portal venous occlusion?
A. Antegrade flow in the portal vein
B. Expansion of the main portal vein diameter
C. Malignant thrombosis
D. Collateral vessels converging to flow into the portal system
E. Cavernous transformation of the portal vein
Answers and Explanations
Question 1
A. Correct! Findings in this case include a nodular, undulating contour of the liver, consistent with cirrhosis. There is also ascites, and the spleen is enlarged.
Other choices and discussion
B. Patients with cirrhosis are at an increased risk for hepatocellular carcinoma (HCC), and thus commonly have screening examinations. However, no mass lesion is present in this case.
C. Acute hepatitis may present as an enlarged liver with diffusely hypoechoic echotexture. The portal triads remain echogenic, giving the “starry sky” appearance.
D. Patients with cholangitis may present with signs of biliary obstruction, including ductal dilation, thickening, and biliary sludge.
E. No masses are seen on this exam.
Question 2
A. Correct! HCC is the most common hepatic malignancy associated with cirrhosis. In the western hemisphere, HCC is commonly associated with chronic hepatitis B and C infections, alcohol use, and cirrhosis.
Other choices and discussion
B. Fibrolamellar carcinoma is a distinct hepatic malignancy that is less common than HCC. It usually occurs in young adults in the second and third decades of life.
C. Angiosarcoma is a rare malignancy that is sometimes associated with toxic agents such as Thorotrast and polyvinyl chloride.
D. Cavernous hemangiomas are the most common benign hepatic neoplasm. The incidence is high, with some studies reporting hemangiomas in up to 20% of the population. These commonly present on ultrasound as small hyperechoic lesions with increased through transmission. They have no malignant potential.
E. Focal nodular hyperplasia is a benign hepatic mass and is more common in females than males. Imaging characteristics often include a central scar on computed tomography and magnetic resonance imaging, early arterial phase enhancement, and delayed uptake on hepatocyte-specific contrast magnetic resonance imaging.
Question 3
E. Correct! Cavernous transformation usually occurs in the setting of longstanding portal venous thrombosis. The characteristic appearance of this condition is the presence of numerous small vessels at the porta hepatis due to collateral circulation.
Other choices and discussion
A. In the setting of portal hypertension or venous occlusion, portal vein flow is away from the liver. This is referred to as retrograde or hepatofugal flow.
B. The main portal vein does not expand with longstanding thrombosis.
C. Malignant thrombosis can be seen in the setting of HCC. However, isolated chronic venous thrombosis does not itself lead to malignancy. Doppler ultrasound can be used to differentiate malignant thrombus (which may have flow) from bland thrombus (which does not have flow).
D. Multiple collateral vessels arise in the setting of longstanding venous occlusion. However, these vessels divert flow away from, not toward, the portal system.
Suggested Readings
Amitrano L, Guardascione MA, Brancaccio V, et al. Risk factors and clinical presentation of portal vein thrombosis in patients with liver cirrhosis. J Hepatol 2004;40:736–741 Guichelaar MM, Benson JT, Malinchoc M, et al. Risk factors for and clinical course of non-anastomotic biliary strictures after liver transplantation. Am J Transplant 2003;3:885–890 Trichopoulos D, Bamia C, Lagiou P, et al. Hepatocellular carcinoma risk factors and disease burden in a European cohort: a nested case-control study. J Natl Cancer Inst 2011;103:1686–1695 Van Gansbeke D, Avni EF, Delcour C, et al. Sonographic features of portal vein thrombosis. Am J Roentgenol 1985;144:749–752Top Tips
Findings of portal hypertension include cirrhosis, splenomegaly, and ascites.
Patients with cirrhosis have an increased risk for developing HCC and are typically routinely screened with ultrasound.
Malignant thrombus may demonstrate vascular flow on Doppler.
Essentials 8
Case
A 70-year-old man with pulsatile groin mass following cardiac catheterization. Longitudinal image of the right femoral artery with Doppler (a) and spectral Doppler image of the right femoral vessels (b) are shown.

Questions
1. Which ONE of the following is the most likely diagnosis?
A. Femoral artery stenosis
B. Femoral artery occlusion
C. Normal waveform
D. Pseudoaneurysm
E. True aneurysm
2. Which of the following choices is (are) reasonable INITIAL steps in the management of this disorder, assuming a clinically stable patient? (Select ALL that apply.)
A. Ultrasound-guided compression
B. Ultrasound-guided thrombin injection
C. Covered stent placement
D. Surgical excision and re-anastomosis
E. Balloon angioplasty
3. Which ONE of the following is a common Doppler imaging finding of a pseudoaneurysm sac?
A. Low systolic velocity
B. Constant unidirectional flow
C. “Yin-yang” appearance
D. Parvus et tardus waveform
E. Low resistance waveform
Answers and Explanations
Question 1
D. Correct! This is a pseudoaneurysm. Spectral Doppler performed over the neck of the aneurysm demonstrates flow both above and below the baseline on the Doppler spectrum.
Femoral pseudoaneurysms are commonly iatrogenic and secondary to arterial catheterization.
Other options and discussion
A. No stenosis is seen.
B. Flow is present.
C. A normal peripheral arterial waveform has a rapid upstroke with systole and a lower velocity with diastole. Flow is not normally reversed (unlike the test case, which shows diastolic signal below baseline).
E. A true aneurysm is a dilatation involving all three vascular layers and would not have the waveform shown here.
Question 2
A. Correct! Direct manual compression performed using the ultrasound transducer is a reasonable first-line treatment. It should be performed for approximately 30 minutes.
B. Correct! Ultrasound-guided injection of 1000 units of thrombin into the pseudoaneurysm sac is a reasonable first-line treatment.
Other choices and discussion
C. Covered stent placement is not routinely performed as initial therapy.
D. Surgical re-anastomosis is not routinely performed as initial therapy.
E. Angioplasty is not indicated.
Question 3
C. Correct! The “yin-yang” appearance is typical of a pseudoaneurysm. This appearance results from bidirectional flow in the aneurysm sac with swirling of contents.
Other choices and discussion
A. Velocities are elevated within the pseudoaneurysm.
B. Flow is typically bidirectional with to-and-fro flow through the neck of the pseudoaneurysm.
C. Parvus et tardus waveform is seen in the setting of arterial stenosis, not pseudoaneurysm.
D. Low resistance waveforms are seen with arteriovenous fistulas. These can result from puncture of artery and vein.
Suggested Readings
Foshager MC, Finlay DE, Longley DG, et al. Duplex and color Doppler sonography of complications after percutaneous interventional vascular procedures. Radiographics 1994;14:239–253 Kreuger K, Zaehringer M, Strohe D, et al. Postcatheterization pseudoaneurysm; results of US-guided thrombin percutaneous injection in 240 patients. Radiology 2005;236:1104–1110Top Tips
A “yin-yang” appearance is seen in a pseudoaneurysm sac due to swirling turbid flow.
Waveform analysis over the neck of a pseudoaneurysm shows bidirectional flow, indicated by signal both above and below the baseline.
Pseudoaneurysms that are symptomatic and/or are > 2 cm are frequently treated.
Essentials 9
Case
A 65-year-old man with microscopic hematuria. Longitudinal image of the right kidney with Doppler (a) and grayscale longitudinal image of the right kidney (b) are shown.

Questions
1. Which ONE of the following is the most likely diagnosis?
A. Dromedary hump
B. Nephrolithiasis
C. Renal cell carcinoma
D. Hydronephrosis
E. Angiomyolipoma
2. What is the most common subtype of renal cell carcinoma?
A. Clear cell
B. Papillary
C. Chromophobe
D. Collecting duct
E. Medullary
3. In the absence of distant metastatic disease, what is the stage of disease for renal cell carcinoma once the tumor has invaded the inferior vena cava?
A. Carcinoma in situ
B. Stage I
C. Stage II
D. Stage III
E. Stage IV
Answers and Explanations
Question 1
C. Correct! A solid hypoechoic mass is seen arising from the lower pole cortex. Doppler confirms vascularity in the lesion. This finding on ultrasound should prompt further workup with computed tomography and/or magnetic resonance imaging, and by imaging this is renal cell carcinoma until proven otherwise.
Other choices and discussion
A. A dromedary hump is a contour variant of the renal cortex, which may mimic a mass lesion. The images shown in the test case demonstrate a discrete renal mass. For problem cases, a nuclear medicine renal scan can sometimes be used to confirm normal renal tissue within a dromedary hump.
B. No calculi are visualized. Renal calculi are highly echogenic and often demonstrate posterior acoustic shadowing. When Doppler is applied over a calculus, there is a characteristic “twinkle” artifact.
D. The collecting system is not dilated.
E. An angiomyolipoma is typically a hyperechoic mass on ultrasound.
Question 2
A. Correct! Clear cell is the most common subtype of renal cell carcinoma, accounting for over 70% of cases. Incidence rates of RCC are increased in patients with von Hippel-Lindau syndrome and in the setting of acquired renal cystic disease (seen in patients who have received long-term dialysis).
Other choices and discussion
B. Papillary carcinoma is the second most common subtype and accounts for approximately 10% of RCC. This subtype is typically slower growing and has a more favorable prognosis than clear cell RCC.
C. On computed tomography and magnetic resonance imaging evaluation, chromophobe carcinomas demonstrate less enhancement and have a more favorable prognosis than clear cell RCC.
D. Collecting duct RCC is a rare and aggressive subtype, accounting for < 1% of RCC.
E. Medullary carcinoma is a rare and aggressive subtype, most commonly found in African-American males with sickle cell disease.
Question 3
D. Correct! This is stage III. Renal vein and inferior vena cava invasion are classified as T3. In the absence of distant metastasis, this renders a stage III classification.
Other choices and discussion
There is no in situ classification of RCC. Staging is as follows:
Stage I: T1 lesion (≤ 7 cm, limited to the kidney) without nodal or distant metastases
Stage II: T2 lesion (≤ 10 cm, limited to the kidney) without nodal or distant metastases
Stage III: T3 lesion without nodal or distant metastases
Stage IV: T4 lesion (spread beyond Gerota fascia and/or invasion of the ipsilateral adrenal gland), or the presence of distant metastatic disease with any primary lesion
Suggested Readings
American Joint Committee on Cancer. Kidney. In: American Joint Committee on Cancer Staging Manual. New York: Springer; 2009: 447 Coogan CL, McKiel CF Jr, Flanagan MJ, et al. Renal medullary carcinoma in patients with sickle cell trait. Urology 1998;51:1049–1050 Patard JJ, Leray E, Rioux-Leclercq N, et al. Prognostic value of histologic subtypes in renal cell carcinoma: a multicenter experience. J Clin Oncol 2005;23:2763–2771Top Tips
Clear cell is the most common subtype of RCC.
Chromophobe RCC demonstrates less enhancement and has a more favorable prognosis than clear cell RCC.
Invasion of the inferior vena cava is classified as a T3 lesion. Extension into the ipsilateral adrenal gland is classified as a T4 lesion.
Essentials 10
Case
A 45-year-old man presents with palpable mass in the scrotum. Grayscale longitudinal image of the left testicle (a) and transverse image of the left testicle with Doppler (b) are shown.

Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


