, Leonid Tiutin2 and Thomas Schwarz3
(1)
Russian Research Center for Radiology and Surgery, St. Petersburg, Russia
(2)
Department of Radiology and Nuclear Medicine, Russian Research Center for Radiology, St. Petersburg, Russia
(3)
Department of Nuclear Medicine Division of Radiology, Medical University Graz, Graz, Austria
Abstract
Melanoma is a relatively rare malignant tumor. Its share among all the oncological diseases makes up only 1.0–1.5%. However, for the last 10 years a steadfast tendency toward increased melanoma incidence has been observed in the Russian Federation. For example, in 1997 the intensive morbidity index constituted 2.93 per 100,000 of population. By 2007 it corresponded to 4.55 per 100,000 population. So, the index increment made up 4.96% (Merabishvili 2006).
Melanoma is a relatively rare malignant tumor. Its share among all the oncological diseases makes up only 1.0–1.5%. However, for the last 10 years a steadfast tendency toward increased melanoma incidence has been observed in the Russian Federation. For example, in 1997 the intensive morbidity index constituted 2.93 per 100,000 of population. By 2007 it corresponded to 4.55 per 100,000 population. So, the index increment made up 4.96% (Merabishvili 2006).
Skin melanoma develops in people over 30. In most cases melanoma develops in the site of a pigmented nevus or birthmark. Nevi appear in childhood; they increase in size with growth of the organism and as a rule stop their growth after the puberty period. Subsequently birthmarks usually undergo depigmentation and fibrosation. Among the factors contributing to malignization of nevi, there are high insolation, different traumas, as well as endocrine and genetic factors (Gantsev 2004).
The clinical picture of melanomas is extremely diverse. Tumors may have different forms, colors, consistency and situation. The dimensions of a malignant neoplasm may vary from several millimeters to many millimeters, but most often they do not exceed 1–3 cm in the maximum dimension. Melanoma may have a round, oval, triangular, polygonal and any other form. The tumor surface may be unchanged, moist or ulcerous, slightly bleeding, or it may be covered with crusts. Skin pattern disappears on the surface of melanoma. The consistency of pathological formation is usually dense, or more seldom elastic. The form of melanoma in this case may be tuberous, nodal, hemispherical or fungiform. Tumor pigmentation has an uneven character of pigment distribution. Several colour combinations may be observed within the same tumor. Melanoma may have different colours – brown, black, blue, pink, violet; but it may be unpigmented as well. There are a number of clinical signs whose occurrence suggests the necessity of advanced patient examination in order to exclude skin melanoma. According to A.I. Paches, they are:
1.
Change in colour of the nevus, its sharp pigmentation (up to a black colour), and in some cases decrease in pigmentation
2.
Uneven coloring
3.
Changed or completely absent skin pattern, desquamation of the nevus
4.
Appearance of an inflammatory areola around the nevus (corolliform redness)
5.
Changed peripheric configuration; for example, blurred contours of the nevus
6.
Increase in size and density of the birthmark
7.
Appearance of small nodulous papillomatous elements with necrosis foci at the base of the nevus
8.
Appearance of itch, burning, pricking and tension in the area of the nevus
9.
Appearance of fissures, ulcers and hemorrhage
17.1 Pathological Anatomy and Mechanisms of Metastases
Currently the neuroectodermal theory of tissular genesis of skin melanoma is most widely recognized. The tumor consists of melanocytes or of nevus cells situated in the basal layer of the epidermis along the dermoepidermal interface. Their main function is synthesis of the melanin pigment, which is taken up and accumulated by epidermal cells.
It is accepted to distinguish three main types of skin melanoma: superficial spreading, nodular and acral-lentiginous melanomas. Two phases are distinguished in melanoma: the horizontal phase, when the disease spreads within the epithelial stratum, and the vertical phase, when malignant cells penetrate into superficial layers of the epidermis with invasion of the basal membrane of the derma and hypodermic fatty tissue. The horizontal phase of superficial spreading melanoma lasts for up to 7 years, while that of acral-lentiginous melanoma lasts for 10–20 years. The vertical phase as a rule is characterized by rapid tumor growth and tendency to metastasis.
In 60% of cases it is superficial spreading melanoma that is observed. Initially it looks like a black or brown pigment spot with diameter no larger than 0.5 cm that does not rise over skin surface. In the vertical phase, heavy tumor growth with formation of an exophytic component takes place. Nodular melanoma is observed approximately in 20% of cases, it is in the form of a node, fungus or polyp of a black or blue-red color. Acral-lentiginous melanoma accompanies Dubrey’s melanosis and constitutes 20% of all skin melanomas. The horizontal phase of pathological formation is long and transition of lentigo to lentiginous melanoma occurs gradually. During malignant transformation, a lentigo acquires an irregular form with scalloped contours and uneven pigment distribution.
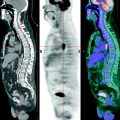
Melanomas metastasize by the lymphogenic route to skin and lymph nodes, and by the hematogenic route to the liver, lungs, brain, bones, kidneys and adrenal glands. The tendencies of the tumor process disseminating depend upon the biological characteristics of a given pathological formation. Some forms are observed which metastasize for a long time only lymphogenically to regional lymph nodes. At the same time, there are melanomas with high malignancy potential, with a tendency to early hematogenic dissemination. Forms of melanomas which metastasize to the skin should be particularly stressed. Among them there are satellite, nodular, erysipeloid and thrombophlebitis-like forms. Satellites are multiple small eruptions situated near the primary focus or at some distance from it in the form of spots retaining the color of the tumor. The nodular form of skin metastases manifests itself as multiple subcutaneous nodes of different size, which may be situated at any distance from the primary formation. The erysipeloid form of skin metastases looks like an area of bluish-red edematous skin surrounding the tumor. The thrombophlebitis-like melanoma manifests itself by radial spreading, painful hardening, enlarged superficial veins and skin hyperaemia around the tumor (Vazhenin et al. 2003).
17.2 Methods of Diagnosis
Diagnosing skin melanoma presents some difficulty. At the beginning of the disease there is no distinct clinical picture, and consequently tumor is hard to distinguish from benign pigment formations. In diagnosing skin melanoma, data of visual examination, palpation, and radioisotopic, thermometrical and morphological methods of examinations are used.
When visually examining a cutaneous covering, it is preferable to use a magnifying glass. Both the tumor itself and the whole skin surface should be examined in order to exclude primary multiple melanoma. The form, size, colour of the tumor and integrity of the epidermis over it are visually assessed.
The primary tumor, surrounding soft tissues and all the lymph nodes available for examination are subjected to palpation. It is necessary in order to determine tumor consistency and the degree of its displacement relatively to subjacent tissues as well as to detect transient, regional and distant metastases of melanoma. Secondary changes in the skin have even edges, round form and dense elastic consistency. Lymph nodes affected by melanoma metastases are enlarged and assume a dense consistency.
Radioisotopic examination is done with twice-substituted sodium phosphate labeled with radioactive phosphorus. The substance is introduced orally on an empty stomach and then radiopharmaceutical (RP) uptake into the tumor and that in the symmetric area of healthy skin are compared by way of contact radiometry. According to some data, RP hyperfixation over a melanoma is four-times as high as that over the contralateral intact area of the epidermis.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


