Skull Base
Addressing normal anatomy, the sphenoid bone forms the foundation of the central skull base. It forms the floor of the middle cranial fossa, provides structure for the cavernous sinus and a base for the pituitary gland. The shape of the sphenoid bone is bird-like with outstretched wings, being composed of the central body, two sets of wings (greater, lesser), and the medial and lateral pterygoid plates (inferiorly). Important foramina include the foramen rotundum, located medially in the anterior greater wing and containing the maxillary nerve (cranial nerve [CN] V2); the foramen ovale, located in the floor of the middle cranial fossa and containing the mandibular nerve (CN V3); and the foramen spinosum, located posterolateral to the foramen ovale and containing the middle meningeal artery and the meningeal branch of the mandibular nerve. The cavernous sinus borders the pituitary gland on each side, and contains medially the internal carotid artery (ICA), with the abducens nerve (CN VI) just inferior and lateral to the ICA.
Laterally, the cavernous sinus contains (from superior to inferior) the oculomotor nerve (CN III), the trochlear nerve (CN IV), and the ophthalmic (CN V1) and maxillary (CN V2) divisions of the trigeminal nerve. Blood flows into the cavernous sinus from the superior and inferior ophthalmic veins, superficial cortical veins, and the sphenoparietal sinus. The drainage of the cavernous sinus is via the superior and inferior petrosal sinuses. The clivus is not properly a separate bone, but rather the gradual sloping bony process that extends from the dorsum sellae to the foramen magnum. The clivus thus includes a portion of the body of the sphenoid bone (basisphenoid) and the basilar (anterior) portion of the occipital bone (basiocciput).
The most important (common) developmental abnormality affecting the middle cranial fossa (and thus by proximity the skull base) is an arachnoid cyst, a lesion that can also be traumatic in origin. By definition, an arachnoid cyst contains cerebrospinal fluid (CSF). It can expand with time. Of all locations, for this entity, the middle cranial fossa is the most common. Bony changes may be present, including thinning and remodeling of the adjacent sphenoid wings.
Meningiomas are the most common benign skull base tumor. One-third of all meningiomas involve the skull base, with most of those involving the sphenoid wing. Bony hyperostosis is not uncommon. For lesions adjacent to the cavernous sinus, it should be kept in mind that sinus invasion is common. Other common locations for a meningioma include the olfactory groove and planum sphenoidale. Pituitary macroadenomas are discussed in depth in Chapter 1, but are relevant to the skull base and surrounding structures due to their propensity for cavernous sinus invasion and optic chiasm compression.
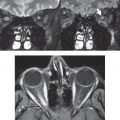
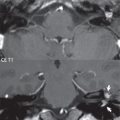
Chordomas and chondrosarcomas are the two malignant tumors of the skull base of note. Chordomas arise from remnants of embryonic notochord, with the second most common location being the clivus (after the sacrum). These are usually midline, destructive, infiltrative, slow-growing tumors and are often large on presentation with a poor prognosis. Areas of dystrophic calcification are common on computed tomography (CT). On magnetic resonance (MR), chordomas appear relatively well-defined and enhance postcontrast ( Fig. 2.1 ). A characteristic feature of this tumor is “thumb-printing” on the anterior brainstem, typically the pons.

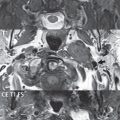
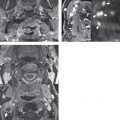
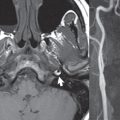
Chondrosarcomas are found along synchondroses, with a propensity to occur in the skull base at the petrooccipital synchondrosis ( Fig. 2.2 ). Thus, these tumors are usually off midline (as opposed to chordomas). Tumor spread is usually by local invasion with destruction of adjacent bone. Calcification is characteristic, but the degree of calcification is widely variable. Resection is often incomplete, and recurrence is common. Increasingly, atypical presentations for lymphoma have been reported, and lymphoma needs to be included in the differential diagnosis of clivus lesions ( Fig. 2.3 ).


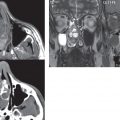
Metastases to the skull base are more common than primary bone tumors. Skull base invasion can also occur secondarily with adjacent malignant tumors—for example, nasopharyngeal carcinoma and, in children, rhabdomyosarcoma ( Fig. 2.4 ). Two other entities to keep in mind, due to some propensity for skull base involvement, are Paget disease and fibrous dysplasia ( Fig. 2.5 ).


Most fractures that involve the skull base are extensions of cranial vault fractures. Thin section CT with bone algorithm reconstruction is the method of choice for evaluation. Clinical presentations include CSF otorrhea/rhinorrhea, hemotympanum, and cranial nerve deficits.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


