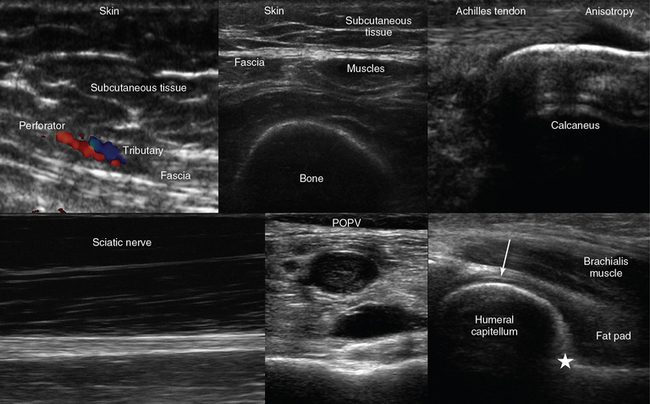
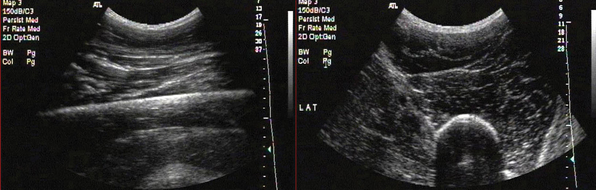
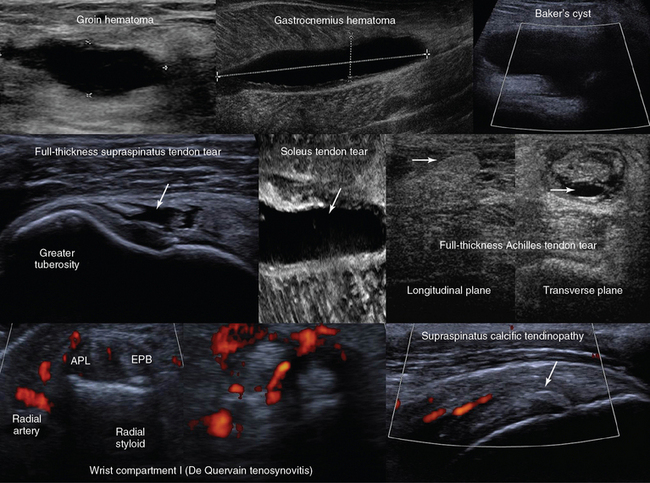
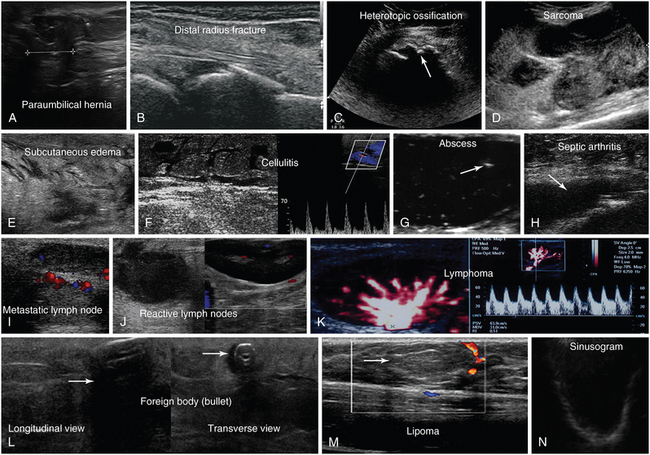
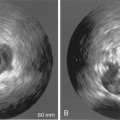
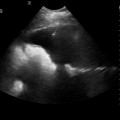
51 ASHOT E. SARGSYAN, GLYKERIA PETROCHEILOU, SERAFIM NANAS, ARIEL L. SHILOH, HEIDI LEE FRANKEL and DIMITRIOS KARAKITSOS Besides encompassing specific focused techniques, the holistic approach (HOLA) ultrasound concept, introduced in Chapter 1, promotes generic scanning of any body part (head-to-toe ultrasound imaging) as modulated by current clinical indications. Any ultrasound view obtained through the skin contains some information about soft tissues. While serving as an imaging window and as anatomic reference structures in focused techniques (e.g., the chest wall in lung scanning), soft tissues per se are often a primary target (e.g., in extremity crush injury). Therefore mastery of fine anatomy is essential for the HOLA-level ultrasound operator, both in terms of tissue type (e.g., fascia, tendon, peritoneum), and in terms of named structures (e.g., basilic vein, gracilis muscle, median nerve). This chapter reviews nonspecific (generic) soft tissue and musculoskeletal (MSK) imaging and miscellaneous intensive care unit (ICU)-relevant HOLA targets. • Visible bruising, swelling, deformity, redness, pulsation, or asymmetry • Palpable mass, warmth, pulsation, crepitus, or other focal abnormality • Known or suspected foreign body, including indwelling access devices • Known or suspected MSK injury or history of a relevant event, such as a fall • Traumatic or surgical wounds • Spontaneous, traumatic, surgically placed, or postsurgical fistulas • Ruling out pathologic lymph nodes • Planning interventional procedures (e.g., vascular access) • Known or suspected vascular pathology or access devices, including status post difficult vascular access Any modern multipurpose system with a high-frequency (7-15 MHz) transducer is appropriate for most superficial targets. Lower frequencies (2-5 MHz) are used for deeper tissues in large subjects or large body parts (e.g., the thigh). More than one transducer can be used on the same region of interest (ROI) to exploit advantages of each. Some experts recommend broadband microconvex transducers (usually 5-8 MHz) for most soft tissue targets because they offer a good balance of resolution and penetration in a wide-angle view through a small footprint. With any transducer, both B-mode and color Doppler mode are often used. Although elastography, an emerging method to map elasticity of tissues, currently has limited use in the ICU, every superficial tissue scanning procedure includes elements of “visual elastography” (see Pathology section later). The uppermost layer of the image is a thin hyperechoic line that corresponds to the skin. Subcutaneous adipose tissue underneath is relatively hypoechoic, with linear echoes (septa). Fascia is a brightly echogenic line (perceived as a contiguous layer during scanning). Muscles appear as hypoechoic structures with organized echogenic fibroadipose septa between fasciculi; the septa merge as the transducer is moved toward a tendon (Figure 51 E-1). Tendons appear hyperechoic and fibrillar when scanning along their course and granular in cross sections; however, even a small deviation from the 90-degree orientation of the ultrasound beams relative to the fibers results in the loss of the echogenic pattern, mimicking a tear or defect. This feature is known as anisotropy (Figure 51-1)—dependence of the imaging pattern on the beam orientation. In tendons, the smooth type-1 collagen fiber bundles are good reflectors (direction dependent) but poor scatterers (direction independent). Peripheral nerves also have a fascicular appearance, but with less anisotropy, and are surrounded by loose connective tissue (see Figure 51-1). Vessels appear as anechoic (black) stripes across the image when the scanning plane aligns with their course. In transverse orientation, arteries are circular and may visibly pulsate. Veins have a near-circular appearance with less prominent walls, easily compress with transducer pressure, but fail to collapse entirely in case of thrombosis (see Figure 51-1). The bone surface is normally depicted as a brightly echogenic line with acoustic shadowing. The joint space is identified by a V-shaped discontinuity in the cortical line from adjacent bones, usually representing fibrocartilaginous tissue (e.g., a meniscus or a labrum). Random collagen fiber orientation in these structures determines their high, nonanisotropic echogenicity.1–3 Hyaline cartilage, on the other hand, looks like a thin hypoechoic rim over the bone (see Figure 51-1). Figure 51-1 Top, left-to-right, Visualization of the skin, subcutaneous tissue, perforator (artery) and tributary (vein) exiting from the hyperechoic abdominal fascia (longitudinal plane); transverse view of the anterior thigh demonstrating the skin, subcutaneous tissue, fascia, muscles, and bone (femur); longitudinal view of the calcanear insertion of the Achilles tendon demonstrating anisotropy. Bottom, left to right, Longitudinal view of the sciatic nerve coursing the posterior thigh; incompressible popliteal vein (POPV) caused by thrombosis; medial sagittal plane of the anterior elbow joint showing the coronoid fossa (star = anterior coronoid recess) and the articular cartilage of the distal humeral epiphysis (arrow). Figure 51 E-1 Longitudinal and transverse anteroposterior images of the thigh. Note the typical structure of a large skeletal muscle in the transverse view. Fascial borders of individual muscles and the compartment can be seen. Note the bright cortical reflection from femur. The hard bony cortex strongly reflects an ultrasonic wave, producing a bright, readily detectable curve or line on the image. This reflection is due to the large acoustic impedance gradient between bone and the overlying soft tissue. Although this makes the internal structure of bone difficult to visualize, it provides a very clear picture of the surface itself and therefore is a sensitive means of fracture detection. Because of the large size of the region of interest (ROI), a low-frequency convex transducer is used. • Change in the relationships, shape, echostructure, or echogenicity of an anticipated (recognized) structure • Focal change within an anticipated structure or its discontinuity • Unexpected response of the structure(s) to transducer compression • Appearance of an extraneous (unanticipated) structure within or between normal structures • Consistent difference between the suspected pathologic area and the presumably normal contralateral site • A trend in any of the above criteria relative to prior examinations Hematomas are collections of extravascular blood caused by common and iatrogenic trauma, coagulation disorders, necrosis, and other mechanisms. They usually appear as poorly demarcated but structurally differing areas within or between anatomic structures, often distorting them (mass effect). A hematoma shows serial changes over time (Figure 51-2). Fresh blood initially looks anechoic and then becomes finely echogenic when clotted. After clot liquefaction, hematomas regain anechoic or hypoechoic appearance with diffuse internal echoes that may form a layer by sedimentation. Most hematomas resolve, but some organize into a chronic hyperechoic mass with echogenic inclusions or concentric layers from repeated bleeds.2–4 Color Doppler ultrasound helps demonstrate deviations of adjacent vessels; it is also helpful in distinguishing between a hematoma and a pathologic tissue. Figure 51-2 Top, left-to-right, Anechoic groin hematoma; gastrocnemius muscle hematoma after clot liquefaction; visualization of a cystic structure (no blood flow is evident) between the medial gastrocnemius and semimembranosus tendon in the popliteal fossa (Baker cyst). Middle, left-to-right, Visualization of a hypoechoic area in the supraspinatus tendon corresponding to a full-thickness tear (arrow); zoom image of a soleus muscle tear (arrow); longitudinal and transverse planes of a full-thickness Achilles tendon tear demonstrating Kager fat pad herniation (arrow) and a hypoechoic hematoma enhancing the conspicuity of the tear (arrow), respectively. Bottom, left-to-right, Focal thickening and increased vascularity surrounding the de Quervain tendons at the level of the radial styloid process (de Quervain tenosynovitis); anterior view of the shoulder depicting a thickened and heterogeneous supraspinatus tendon with a focus of calcification (arrow) and increased vascularity (calcific tendinopathy). APL, Abductor pollicis longus; EPB, extensor pollicis brevis. (Images of soleus muscle tear (middle) and de Quervain tendons (bottom) courtesy Dr. K. Stefanidis.) Ultrasound imaging is valuable in musculotendinous injuries as part of the physical examination in trauma. Acute muscle contusion and hemorrhage appear hyperechoic, whereas later stages of injury exhibit mixed patterns. Partial or complete muscle tears with or without retractions are usually obvious (see Figure 51-2). Intramuscular hematomas may later evolve into seromas or intramuscular cysts (anechoic fluid collections) that may require aspiration or surgical drainage. Heterogeneous, grainy muscular patterns with a hypoechoic appearance of septa and fasciae are described in malignant hyperthermia. Hypoechoic muscular swelling with architectural disorganization may be observed in traumatic rhabdomyolysis. Partial and complete tendon tears can be identified by dynamic ultrasound evaluation assessing the tendon’s integrity through the respective range of motion. Hypoechoic-to-anechoic intratendinal regions indicate partial tearing. Full-thickness tears may appear as tendon discontinuity with or without retraction and acoustic shadowing, whereas defects may be filled by hematomas or fat pad herniation (see Figure 51-2). An anechoic fluid cuff around a thickened, hyperechoic tendon with increased vascularity suggests tenosynovitis. Tendinopathy may appear as an intratendinous, hypoechoic patchy or hyperechoic calcific area with increased vascularity and loss of anisotropy and fibrillar pattern (see Figure 51-2). Ganglion cysts arise from the joint capsule or tendon sheaths and appear anechoic. The Baker cyst, first described by Dr. William Baker in 1877, is the most common mass in the popliteal fossa, which represents a fluid-distended gastrocnemio–semimembranosus bursa (see Figure 51-2).3 A cortical discontinuity with step-off deformity is the diagnostic hallmark of a bone fracture that is best seen in a plane perpendicular to the fracture line (Figure 51-3). Intensivists rarely deal with fracture diagnosis because patients arrive with a full set of radiographic imagery or after orthopedic surgery. Ultrasound imaging is relevant for monitoring adjacent soft tissue damage, such as hematomas or joint effusions (hemarthrosis). Monitoring can detect fracture nonunion and other complications (e.g., osteomyelitis) because ultrasound imaging depicts callus formation earlier than radiography, particularly in open injuries.2,3 Heterotopic ossification (HO) is usually observed in periarticular muscles of the limbs, mainly in neurologic states (spinal cord injury, hemiplegia after stroke, or traumatic brain injury) or after burns, trauma, and joint arthroplasty, and it can severely affect the joint’s range of motion. Early clinical features (pain, swelling, erythema, warmth) may resemble skin infection, deep vein thrombosis (DVT), or acute arthritis. Mineralization is detected by ultrasound earlier than in radiography as an inner hypoechoic core surrounded by a peripheral hyperechoic band of mineralized islands (“zone phenomenon”) with increased vascularity. In cases when calcifications have not yet occurred, HO may be confused with sarcomas (see Figure 51-3). Figure 51-3 A, Longitudinal view of a paraumbilical hernia containing omentum (12-mm defect). B, Lateral/coronal long-axis scan of the distal forearm in a trauma patient. Note a comminuted distal radius fracture: four distinct segments of bone with mutual misalignment, with a hypoechoic area of a likely hematoma (note the extensor pollicis brevis tendon across the screen, parallel to the skin, and the general axis of the fractured bone). C, Visualization of the “zone phenomenon” in heterotopic ossification: an inner hypoechoic core is surrounded by hyperechoic mineralized islands (arrow) within the iliopsoas muscle adjacent to the hip joint. D, Heterogeneous groin mass with ill-defined borders (sarcoma). E, Cobblestone appearance of the subcutaneous tissue resulting from generalized interstitial edema in a heart failure patient. F, Cobblestone echotexture of the subcutaneous tissue in a region of the gastrocnemius muscle and depiction of unusually high flow (increased peak systolic Doppler velocity) in a local perforator (cellulitis). G, Zoom image of a subcutaneous hypoechoic abscess with hyperechoic punctiform material. H, hypoechoic knee effusion with echogenic material (arrow, septic arthritis). I, Hypoechoic metastatic arm lymph node in a patient with thyroid cancer. J, Reactive round- and oval-shaped groin lymph nodes. K, Oval-shaped groin lymph node with a Doppler-derived resistive index (RI) 5 0.51 (power Doppler mode), which was initially characterized as reactive, but eventually proved (biopsy) to be malignant (lymphoma) with cystic necrosis. L, Longitudinal and transverse planes of the thigh depicting a bullet casting an acoustic shadow (arrow) and the formation of “halo” (arrow), respectively. M, Longitudinal view of superficial lipoma (arrow) over the xiphoid process. N, Visualization of a totally fluid-filled sinus that appears hypoechoic, with its posterior and lateral walls delineated (sinusogram). (Images in A, courtesy Dr. K. Stefanidis; D, L, and M courtesy Dr. K. Shanbhogue; G, courtesy Dr. J. Poularas.) Recently, ultrasound has been used to determine the type and extent of traumatic nerve injuries
Soft tissue, musculoskeletal system, and miscellaneous targets
Overview
Equipment and technique
Normal patterns
Pathology: High-level considerations
Pathology: Specific types
Related posts:
 Ultrasound-guided peripheral intravenous access
Ultrasound-guided peripheral intravenous access
 Ultrasound-guided arterial catheterization
Ultrasound-guided arterial catheterization
 Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
 Use of ultrasound in the evaluation and treatment of intraabdominal hypertension and abdominal compartment syndrome
Use of ultrasound in the evaluation and treatment of intraabdominal hypertension and abdominal compartment syndrome
 Ultrasound imaging in space flight
Ultrasound imaging in space flight
 Approach to the urogenital system
Approach to the urogenital system
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine
