Abstract
A solitary lucent defect may result from a necrotic cavity, cyst, pneumatocele, or a loculated hydropneumothorax, but of these possibilities, a necrotic cavity is the most common. A necrotic cavity is caused by ischemic necrosis of the lung that may result from a bacterial, tuberculous, or fungal infection. A loculated hydropneumothorax is a complication of empyema with bronchopleural fistula that must sometimes be distinguished from a pulmonary cavity. When a tumor outgrows or invades and destroys its blood supply, it causes a cavitary mass. A cavitary tumor often has a thick nodular wall, but a cavitary tumor cannot be reliably distinguished from a lung abscess based on its radiologic features. A solitary cavity usually requires a bacteriologic or histologic diagnosis.
Keywords
bronchogenic cyst, cavity, coccidioidomycosis, cyst, fungal infections, histoplasmosis, hydropneumothorax, intrapulmonary sequestration, lung abscess, lung cancer, necrotizing pneumonia, pneumatocele, tuberculosis
Questions
- 1.
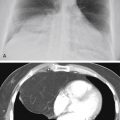
Match the cases shown in Fig. 23.1, A – D , with the following diagnoses:
____Bronchogenic carcinoma.
____Pneumonia with abscess.
____Bronchopleural fistula with hydropneumothorax.
____Pulmonary gangrene.

Fig. 23.1
- 2.
Which one of the following pulmonary infections is least likely cause of necrotizing pneumonia?
- a.
Streptococcus pneumoniae.
- b.
Pseudomonas.
- c.
Klebsiella.
- d.
Staphylococcus aureus.
- e.
Mixed gram-negative pneumonia.
- a.
- 3.
Refer to Fig. 23.2 . Which one of the following diagnoses is least likely?
- a.
Bronchogenic carcinoma.
- b.
Metastatic nasopharyngeal carcinoma.
- c.
Chronic anaerobic abscess.
- d.
Bronchogenic cyst.
- e.
Tuberculous cavity.

Fig. 23.2
- a.
- 4.
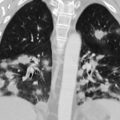
Which one of the following best explains the radiologic presentation in Fig. 23.3, A-C ?
- a.
Metastatic melanoma.
- b.
Tuberculosis with bronchogenic spread.
- c.
Bronchogenic carcinoma.
- d.
Coccidioidomycosis.
- e.
Metastatic nasopharyngeal carcinoma.

Fig. 23.3
- a.
Discussion
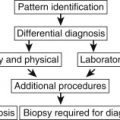
The radiologic presentation of a localized, avascular, lucent lung defect surrounded by a band of opacity might best be described as a hole in the lung, although this is a nonmedical term. Chart 23.1 lists a number of causes for a solitary hole in the lung that differ considerably in their pathogenesis. For this reason, such terms as cavity, cyst, and pneumatocele constitute the differential diagnosis for a hole in the lung. 317 This chapter examines differences in the pathogenesis of these lesions as a basis for understanding the similarities and differences in their radiologic presentations.
- I.
Cavity
- A.
Inflammation
- 1.
Abscess, acute or chronic
- a.
Pyogenic infection 207 (staphylococcal and gram-negative pneumonia)
- b.
Aspiration pneumonia (common source of anaerobes)
- c.
- a.
- 2.
Fungal infection 371
- 3.
Mycobacterial infection
- 1.
- B.
Neoplasms
- 1.
Primary lung tumor 587
- 2.
Metastases (usually multiple) 118
- a.
Squamous cell (e.g., nasopharynx, esophagus, cervix)
- b.
Adenocarcinoma (e.g., lung, breast, gastrointestinal tract)
- c.
Osteosarcoma (rare)
- d.
Melanoma
- a.
- 1.
- C.
Vascular (commonly multiple)
- 1.
- 2.
Granulomatosis with polyangiitis 4
- 3.
Infarct (thromboemboli or septic emboli)
- 1.
- D.
Environmental
- 1.
Silicosis and coal workers’ pneumoconiosis (most commonly owing to complicating tuberculosis)
- 1.
- A.
- II.
Pneumatocele
- III.
- IV.
Parasitic cysts (hydatid cyst) 30 , 435
- V.
Bronchiectatic cyst 464
- VI.
Bullous emphysema 169
Cavity
The radiologic appearance of a pulmonary cavity is the result of necrosis of lung parenchyma with evacuation of the necrotic tissue via the tracheobronchial tree. A communication with the tracheobronchial tree permits air to enter the area of necrosis, with the radiologic result of a lucent defect. The necrosis causes near-complete destruction of the alveolar walls, interlobular septa, and bronchovascular bundles in the area of the cavity, resulting in loss of normal vascular markings throughout the area of lucency. The surrounding normal lung parenchyma reacts to the necrosis by forming a band of inflammation around the necrotic material, with local edema and hemorrhage. When the cavity expands under tension, as frequently happens in patients who are on positive-pressure ventilator therapy, there may even be compression of normal surrounding lung. The surrounding inflammatory cellular infiltrate, edema, hemorrhage, and compressed normal lung all contribute to the cavity wall. Central necrosis of a preexisting nodule or mass with drainage of its liquefied contents is a second mechanism for the development of a cavity. Central necrosis with liquefaction of a pulmonary lesion cannot be detected on a chest radiograph prior to drainage of a portion of the liquid. However, computed tomography (CT) is sensitive to the difference in opacity caused by liquefaction and may be useful for detecting early necrosis of a pulmonary infection or neoplasm ( Fig. 23.4, A and B ).

The radiologic characteristics of the wall of a cavity are determined by the reaction of the lung parenchyma to the pathologic process. A surrounding air space consolidation indicates acute edema, hemorrhage, or exudate, whereas irregular reticular strands are suggestive of chronic fibrotic scars. Therefore, wall characteristics may be helpful in establishing the age of the cavity. In addition, necrosis of an inflammatory or neoplastic mass may leave thick nodular walls ( Fig. 23.5, A and B ; see Fig. 23.1, A ).

Pyogenic Infection
The term abscess is usually reserved for cavities that are caused by pyogenic infections. This complication indicates a virulent process that results in vasculitis with thrombosis of small vessels, which leads to necrosis of lung tissue. The abscess, which is made up of necrotic material, will appear to be of tissue opacity until communications with airways are established. These communications permit drainage of the necrotic debris. This liquefied necrotic material is coughed up, with the radiologic result of a lucent defect or cavity. The presence of cavitation in the acute phase of a pulmonary infection is a significant radiologic finding that narrows the differential considerations; viral and mycoplasma pneumonia are virtually eliminated, and pneumococcal pneumonia (infection with Streptococcus pneumoniae ) would be a rarity. The organisms most likely to lead to cavitation are Staphylococcus , beta-hemolytic streptococci, Klebsiella, Pseudomonas, Escherichia coli, mixed gram-negative organisms, and anaerobes. (Answer to question 2 is a .)
Aspiration is frequently the source of the mixed gram-negative and anaerobic infections. This may be the result of subclinical aspiration and has been described as gravitational pneumonia. Aspiration pneumonia should be particularly suspected when the cavity occurs in a dependent portion of the lung. The clinical setting of a condition such as poor oral hygiene, alcoholism, or a tumor in the nasopharynx, larynx, or mouth supports the diagnosis. The patient typically experiences a febrile response with productive cough, similar to that of other patients with necrotizing pneumonia.
On occasion, the cavities resulting from a necrotizing pneumonia rupture into the pleura, forming a bronchopleural fistula. This leads to the radiologic appearance of a hydropneumothorax, which is usually recognized by an air-fluid level in the pleural space. Pleural air-fluid collections are often elliptic, may lack an identifiable wall, and have air-fluid levels that differ in length depending on the radiographic projection. Abscesses tend to have spherical thick walls and air-fluid levels that are equal in length, regardless of the radiographic projection 458 , 519 , 557 ( Fig. 23.6, A and B ; see Fig. 23.1, C and D ). CT may be required to distinguish an abscess from a loculated hydropneumothorax secondary to bronchopleural fistula. 318 , 625 The clinical presentation of pyogenic pneumonia is usually dramatic with the patient being profoundly ill, running a toxic febrile course, and having an elevated white blood cell (WBC) count. Because of the necrosis of lung tissue, hemoptysis is not a rare complication of these more virulent infections. Culture of the organism is required for definitive diagnosis.

Pulmonary gangrene 662 results from the very acute ischemic necrosis of lung tissue. It differs from lung abscess in that a region of lung undergoes necrosis, detaches from viable lung, and forms a mass of devitalized tissue lying within a cavity. Organisms to be considered when gangrene is identified include Staphylococcus aureus, Streptococcus spp., Klebsiella pneumoniae, Haemophilus influenzae, Mucor fungi, and Aspergillus. The characteristic radiographic appearance is that of a mass surrounded by eccentric lucency (see Fig. 23.1, B ). Radiographically, pulmonary gangrene may resemble a fungus ball in a cavity, but the latter is due to a solid mass of fungus that has colonized a preexisting cavity or cystic space. CT may be helpful in demonstrating that the intracavitary mass consists of lung. Early diagnosis of gangrene is important because it may require surgical resection.
Granulomatous Disease
Tuberculosis is the prototypical cause of an infectious pulmonary cavity. The cavitary phase of tuberculosis rarely occurs at the time of the initial infection but is a secondary phenomenon resulting from a hyperimmune response. 82 , 641 The necrosis of lung tissue liberates organisms previously isolated by a surrounding fibrotic reaction. The cavities of tuberculosis are usually quite distinctive because of their proclivity to the apical or the posterior segments of the upper lobes. Approximately 10% of tuberculous cavities are found in atypical locations. A cavity in an anterior segment of an upper lobe as the sole manifestation of pulmonary tuberculosis is very rare. Isolated lower lobe cavities are rarely caused by tuberculosis, but lower lobe tuberculosis in association with upper lobe disease is not rare. Although these latter locations should be considered more suggestive of some of the other causes of cavitary disease, such as acute necrotizing pneumonias or fungal infections, an unusual location should not be cause for rejecting the diagnosis of tuberculosis (see Fig. 23.5 ). 54 , 82 , 215 , 388 , 641
Other radiologic features that aid in the identification of a tuberculous cavity include the following: (1) associated reticular pulmonary scars; (2) volume loss in the involved lobe; (3) pleural thickening; (4) pleural calcification; and (5) calcified hilar or mediastinal lymph nodes. These are all the result of a long-standing inflammatory response. The reticular or linear scars cause a very irregular margin of the outer wall of the cavity. These linear opacities are the result of granulomas and fibrotic scarring. The fibrotic scars are also the cause of the volume loss, which is radiologically detected by noting an elevation of the hilum and shift of the mediastinum (see discussion of cicatrizing atelectasis in Chapter 13 ). Calcified nodular opacities in the area of the cavity indicate a previous granulomatous infection. Associated homogeneous nodules are less diagnostic but may occur in clusters and indicate transbronchial spread of infection.
Reactivation of tuberculosis indicates a failure in host defenses. Older patients and those with chronic illnesses, including acquired immunodeficiency syndrome (AIDS) and a variety of neoplasms 342 —in particular, lung cancer, leukemia, and lymphoma—are at increased risk for developing active tuberculosis. The failure of an immune response results in liberation of organisms that may have been isolated for years. Exposure to a person with cavitary tuberculosis accounts for most new cases of tuberculosis. In addition to the possibility of spreading the infection to others, patients in this phase of tuberculosis are at considerable risk of developing disseminated infection, which may be bronchogenic or hematogenous.
The distinction of hematogenous and bronchogenic spread is greatly assisted by assessment of the clinical course. Involvement of multiple organs indicates hematogenous or miliary infection. As described in Chapter 17 , the radiologic presentation of miliary tuberculosis is that of a diffuse fine nodular pattern, with the nodules being sharply defined. The association of cavitary tuberculosis with disseminated larger opacities in the range of 2 to 5 mm and that have ill-defined borders is more suggestive of bronchogenic spread, with the opacities representing peribronchial inflammatory infiltrates and exudation into the terminal air spaces. The latter has been termed acinar tuberculosis. 175 The combination of a large, irregular, upper lobe cavity and ill-defined opacities in the lower lobe strongly suggests the diagnosis. A primary or secondary tumor is unlikely to produce such a pattern; the irregular nodules with ill-defined borders are certainly not typical metastatic nodules. Bronchogenic carcinoma might produce a similar cavity but is an unlikely cause for the disseminated opacities. Coccidioidomycosis is a granulomatous infection that can mimic tuberculosis and cannot be entirely eliminated by radiologic criteria alone, but the case shown in Fig. 23.3, A-C , would not represent a classic appearance for cavitary coccidioidomycosis and is a case of cavitary tuberculosis with transbronchial spread of the infection. (Answer to question 4 is b. )
Atypical mycobacterial infections ( Fig. 23.7, A and B ) produce a variety of patterns including cavities that are indistinguishable from tuberculosis, nodules, masses, and bronchiectasis, as well as the small diffuse nodules of hypersensitivity pneumonitis. Mycobacterium avium complex (MAC) is the most common of the nontuberculous mycobacteria. When conventional laboratory examinations fail to isolate the cause of an apical cavity, atypical mycobacteria must be considered. Although the radiologic features of the cavity are often identical to those in typical tuberculosis, some differences in the radiologic presentation of the two infections have been described. The atypical organisms are more likely to produce multiple, thin-walled, apical cavities with only minimal surrounding parenchymal disease and with minimal or no pleural reaction. Nodules surrounding a cavity are uncommon. Nodules or masses without a cavity may mimic the appearance of lung cancer or metastases. Patients with chronic lung diseases, including chronic obstructive pulmonary disease, interstitial lung disease, cystic fibrosis, and bronchiectasis, are at increased risk for atypical mycobacterial infection. MAC is also a common cause of opportunistic infection, especially in patients with AIDS. It occurs in the setting of a CD4 count of less than 100 cells/mm 3 and causes cavities, nodules, endobronchial nodules, pericardial effusion, and extensive hilar or mediastinal adenopathy. 366