Tend to be fusiform in shape, without a defined neck (as seen commonly with intracranial aneurysms)
Often unrelated to arterial branching sites
Clinical Issues
• Presenting symptoms include back pain, headache, vomiting, weakness, paraparesis, and paralysis
• Treatment may include clipping if neck is present or trapping with occlusion of parent vessel or wrapping with muslin
• Isolated reports of coil embolization of spinal aneurysms
• Spontaneous regression reported in aneurysms with inflammatory etiology
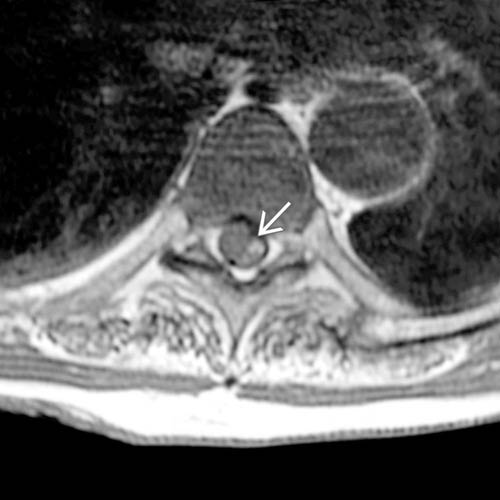
(Left) Axial T1WI MR shows high signal intensity blood throughout the subarachnoid space in this patient with spinal aneurysm.
(Right) Anteroposterior catheter angiography with injection of left-sided intercostal artery shows filling of a small anterior spinal aneurysm .
(Left) Lateral catheter angiography with injection of the thoracolumbar intercostal artery shows filling of a fusiform anterior spinal artery aneurysm .
(Right) Anteroposterior catheter angiography 3D spin study shows small outpouching of contrast off of the ventral medial aspect of the left vertebral artery, due to an aneurysm at the origin of the anterior spinal artery . There is a small amount of reflux extending down the right vertebral artery .
TERMINOLOGY
Definitions
• Fusiform or saccular dilatation of artery supplying spinal cord, particularly anterior spinal artery (ASA) but including radiculomedullary branches
IMAGING
General Features
• Best diagnostic clue
Catheter angiographic finding of aneurysm in setting of spinal subarachnoid hemorrhage
• Location
Intradural extramedullary location, primarily along ventral cord surface
• Size
Variable, but generally small (3 mm)
• Morphology
Fusiform or saccular
MR Findings
• T1WI
Increased T1 signal from CSF due to subarachnoid hemorrhage (may be near isointense if acute)
Only gold members can continue reading. Log In or Register to continue

 in this patient with spinal aneurysm.
in this patient with spinal aneurysm.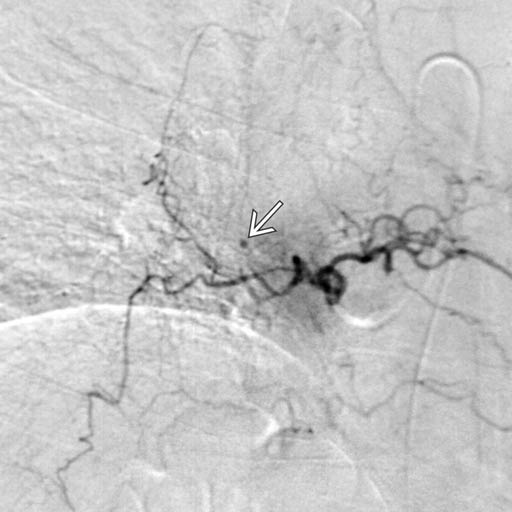
 .
.
 .
.
 . There is a small amount of reflux extending down the right vertebral artery
. There is a small amount of reflux extending down the right vertebral artery  .
.










