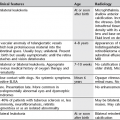
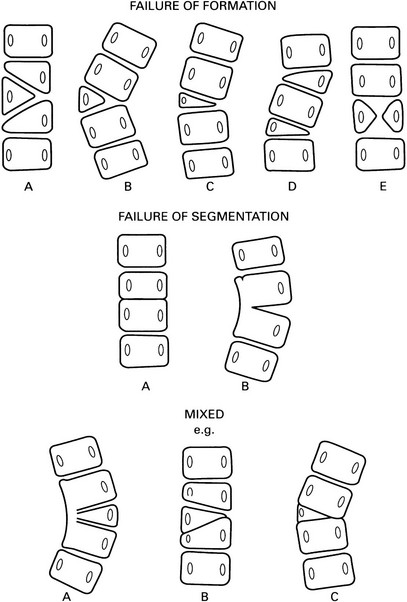
2 2.1 Scoliosis 2% prevalence for curves > 10°. 1. Infantile – diagnosed before the age of 4 years. 90% are thoracic and concave to the right. More common in boys. 90% resolve spontaneously. 2. Juvenile – diagnosed between 4 and 9 years. More common in girls. Almost always progressive. 3. Adolescent – diagnosed between 10 years and maturity. More common in females. Majority are concave to the left in the thoracic region. Prognosis is dependent on the anatomical abnormality and a classification (see figure on p. 37) is, therefore, important. A Incarcerated hemivertebra – a straight spine with little tendency to progression. B Free hemivertebra – may be progressive. C Wedge vertebra – better prognosis than a free hemivertebra. D Multiple hemivertebrae – failure of formation on the same side results in a severe curve. Hemivertebrae on opposite sides may compensate each other. A Bilateral → block vertebra and a short spine, e.g. Klippel–Feil. B Unilateral unsegmented bar – severely progressive curve with varying degrees of kyphosis or lordosis depending on the position of the bar. A Unilateral unsegmented bar and a hemivertebra – severely progressive. B Partially segmented incarcerated hemivertebra. C Bilateral failure of segmentation incorporating a hemivertebra. Indicators of serious progression are: 1. Neurofibromatosis* – in up to 40% of patients. Classically a sharply angled short segment scoliosis with a severe kyphosis. The apical vertebrae are irregular and wedged with adjacent dysplastic ribs. 25% have a congenital vertebral anomaly. 2. Marfan’s syndrome* – scoliosis in 40–60%. Double structural curves are typical. 3. Homocystinuria* – similar to Marfan’s syndrome. 4. Other skeletal dysplasias – spondyloepiphyseal dysplasia congenita, spondyloepimetaphyseal dysplasia, pseudoachondroplasia, metatropic dwarfism, diastrophic dwarfism, Kniest disease, spondylocostal dysostosis. A flexible lumbar curve, convex to the side of the shorter leg. Disparity of iliac crest level. 1. Osteoid osteoma* – 10% occur in the spine. A lamina or pedicle at the apex of the curve will be sclerotic or overgrown. 3. Intraspinal tumour (see 2.16). 2.2 Solitary collapsed vertebra (a) Metastasis – breast, bronchus, prostate, kidney and thyroid account for the majority of patients with a solitary spinal metastasis. The disc spaces are preserved until late. The bone may be lytic, sclerotic or mixed. ± Destruction of a pedicle. (b) Multiple myeloma/plasmacytoma* – a common site, especially for plasmacytoma. May mimic an osteolytic metastasis or be expansile and resemble an aneurysmal bone cyst. 2. Osteoporosis (q.v.) – generalized osteopenia. Coarsened trabecular pattern in adjacent vertebrae due to resorption of secondary trabeculae. 4. Infection – with destruction of vertebral end-plates and adjacent disc spaces. 5. Langerhans’ cell histiocytosis* – eosinophil granuloma is the most frequent cause of a solitary vertebra plana in childhood. The posterior elements are usually spared. 6. Benign tumours – haemangioma, giant cell tumour and aneurysmal bone cyst. 7. Paget’s disease* – diagnosis is difficult when a solitary vertebra is involved. Neural arch is affected in most cases. Sclerosis and expansion. If other non-collapsed vertebrae are affected then diagnosis becomes much easier. 2.3 Multiple collapsed vertebrae 2. Neoplastic disease – wedge fractures are particularly related to osteolytic metastases and osteolytic marrow tumours, e.g. multiple myeloma, leukaemia and lymphoma. Altered or obliterated normal trabeculae. Disc spaces are usually preserved until late. Paravertebral soft-tissue mass is more common in myeloma than metastases. 3. Trauma – discontinuity of trabeculae, sclerosis of the fracture line due to compressed and overlapped trabeculae. Disc space usually preserved. The lower cervical, lower dorsal and upper lumbar spine are most commonly affected. Usually no soft-tissue mass. MRI usually shows the end-plates to be spared, cf. pyogenic infection. 4. Scheuermann’s disease – irregular end-plates and numerous Schmorl’s nodes in the thoracic spine of children and young adults. Disc-space narrowing. Often progresses to a severe kyphosis. Secondary degenerative changes later. 5. Infection – destruction of end-plates adjacent to a destroyed disc. 6. Langerhans’ cell histiocytosis* – the spine is more frequently involved in eosinophilic granuloma and Hand–Schüller–Christian disease than in Letterer–Siwe disease. Most common in young people. The thoracic and lumbosacral spine are the usual sites of disease. Disc spaces are preserved. 7. Sickle-cell anaemia* – characteristic step-like depression in the central part of the end-plate.
Spine
Idiopathic
Congenital
Mesodermal and neuroectodermal diseases
Leg length discrepancy
Painful scoliosis
Radiology Key
Fastest Radiology Insight Engine