CHAPTER 96 Subclavian Steal Syndrome
The aortic arch extends from approximately the level of the upper border of the second sternocostal articulation on the right, runs superiorly, posteriorly, and to the left in front of the trachea, where it then turns posteriorly left of the trachea and finally inferiorly on the left side of the body. The branches that conventionally arise from the arch are the right brachiocephalic artery, the left common carotid artery, and the left subclavian artery (see Chapter 71).
DEFINITION
Subclavian steal syndrome is defined as stenosis or occlusion of the subclavian artery proximal to the origin of the vertebral artery, with consequent reversal of blood flow in the vertebral artery to supply the distal subclavian artery, resulting in neurologic symptoms. This reversal of flow is said to “steal” blood from the intracranial circulation, which can cause ischemia or stroke.1 In the absence of neurologic symptoms, the constellation of findings can be called subclavian steal phenomenon.
ETIOLOGY AND PATHOPHYSIOLOGY
Atherosclerosis is the most common cause of subclavian steal syndrome. Although Takayasu arteritis is an infrequent cause of the syndrome, it occurs more commonly in people of Asian descent.2
Vollmar and colleagues3 have described four categories of subclavian steal phenomenon based on the vascular territories that provide and receive flow—vertebrovertebral, carotid-basilar, external carotid-vertebral, and carotid-subclavian. Another classification scheme4 is based on the degree of hemodynamic disturbances of the vertebral artery: stage I (occult steal, decreased blood flow), stage II (partial steal, transient or partial reversal of flow), and stage III (complete steal, permanent reversal of flow).
When the collateral flow directs a large amount of flow into the subclavian artery and away from the brain, neurologic symptoms can occur. Such symptoms have been reported to occur in approximately 36% of patients.5 Often, the circle of Willis can provide enough collateral circulation to the brainstem to avert neurologic symptoms. If the posterior communicating artery is stenotic, occluded, or absent, or if there is concomitant carotid disease, then neurologic symptoms are more likely to occur.
MANIFESTATIONS OF DISEASE
Clinical Presentation
Most patients with reversal of flow in the vertebral artery have neurologic symptoms.5 In the absence of neurologic symptoms, patients are said to have subclavian steal phenomenon.
Neurologic symptoms of subclavian steal syndrome include lightheadedness, dizziness, vertigo, upper extremity numbness, visual alterations, transient ischemic attacks and, rarely, seizures or stroke.6–8 Ipsilateral upper extremity exercise increases the blood flow demand in the subclavian artery and can cause transient neurologic symptoms caused by an increase in diversion of intracranial blood flow.9
On physical examination, subclavian steal may manifest with a subclavian artery bruit or reduced blood pressure in the ipsilateral upper extremity, along with weakness of the radial pulse.10
Imaging Techniques and Findings
Ultrasound
Sonography is the initial imaging examination when subclavian steal syndrome is suspected. Ultrasound with pulsed Doppler spectral analysis can demonstrate patency and flow direction in the vertebral artery and can establish the presence of subclavian steal.11,12
Subclavian steal phenomenon is associated with specific vertebral artery waveforms. There are four types of waveforms that indicate the degree of abnormal hemodynamics11:
In occult steal (Branchereau stage I),4 the pulsed wave Doppler spectrum typically demonstrates antegrade vertebral flow with midsystolic deceleration.11,12 The waveform may show a reversed late systolic flow as a response to reactive hyperemia in the upper extremity after arm exercise (see Fig. 96-1B). In partial subclavian steal (stage II), pulsed wave Doppler depicts partial flow reversal. The Doppler waveform in occult and partial subclavian steal has been described as the bunny rabbit sign because of its resemblance to the outline of a rabbit (Fig. 96-1A).11,12
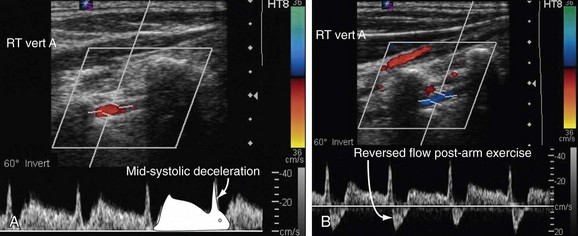
 FIGURE 96-1
FIGURE 96-1


