Linear structural discontinuities may be observed at the level of the inner table, outer table, or diploë, or may entail the full thickness of the calvaria.
Table 4.3 Linear lucencies
Diagnosis
Findings
Normal vascular channels
Tortuous course, branching, with sclerotic and smooth borders and little radiographic contrast; different from the straight or zig-zag pattern of sharp fracture lines.
Arteries
Middle meningeal artery (inner table) located behind the coronal suture, often the superior and occipital branching is radiographically visible.
The superficial and posterior temporal arteries run vertically in the temporal squama (outer table); they are rarely visible but can mimic a fracture. The supraorbital artery courses vertically in the outer table.
Veins
The broad sphenoparietal groove of the bregmatic vein (a meningeal vein) is clearly visible as it runs downward from the bregma in the inner table, taking a rather tortuous course behind and parallel to the coronal suture. The channels of the meningeal vessels become better visible at a later (school) age.
Venous sinuses
Inner table is traversed by broad, deep, nontortuous channels that appear by approximately 3 y of age. The sagittal sinus drains occipitally into the confluence sinus (torcula herophili) along with the transverse sinus and straight sinus (not visible). The right transverse sinus is often wider than the left.
Diploic veins
These vessels typically have a stellate configuration in the parietal bone and form “varix nodes” or “lakes” that appear as radiolucencies.
Several fine diploic veins are sometimes visible in the frontal squama of infants.
Emissary veins
These connect the venous sinuses with the extracranial veins. They show a well-defined “vermiform” configuration in the calvaria and perforate it through smooth-edged foramina: the frontal (supraorbital) emissary vein; the mastoid emissary vein; the occipital emissary vein, which traverses one or more foramina in the midline at the internal occipital protuberance; and the parietal emissary vein, which traverses small, rarely visible, parietal foramina next to the sagittal suture in the posterior third. Emissary veins are uncommon in the area of the former metopic suture but may occur along its course to a point above the crista galli.
Abnormal vascular channels Diploic hyperplasia in hemolytic anemia and cyanotic heart disease
Vascular channels are widened and show increased tortuosity.
Craniostenosis
Markedly wide and deep vascular channels.
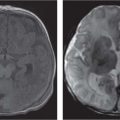
Fig. 4.5a–c Sinus pericranii. (a) The lump in the left parieto-occipital region of 2-year-old boy is thought to be a dermoid. On T1-weighted image, it is isointense to gray matter. (b) On T2-weighted image, it is hyperintense. (c) There is little enhancement after gadolinium (Gd).
Fractures
In normal fracture union, the fracture line widens slightly and is thus more “visible” around 3 to 5 days after trauma, then its margins become indistinct. This is due to osteoclastic resorption of the debris, followed by osteoblastic repair.
Fracture malunion (“growing” fracture, see Fig. 4.9a–c) is marked by progressive widening of the fracture line (most common with burst fractures) and a protracted “hematoma” (cerebrospinal fluid [CSF] pulsations) with bridging of the fracture site by connective tissue, due to a dural tear.
Lines that mimic a fracture include the following:
Metopic suture
Posterior intraoccipital synchondrosis
Mendosal suture
Accessory suture in the parietal bone
Wormian bones
Only gold members can continue reading. Log In or Register to continue