CHAPTER 10 Symptoms of lower gastrointestinal disease
Introduction
Gastrointestinal symptoms are very common within the general population (Thompson et al., 2003). There is a high prevalence of rectal bleeding (Crossland and Jones, 1995; Thompson et al., 2000), change in bowel habit (Everhart et al., 1989) and abdominal pain (Sandler, 1990). Since any one of these symptoms alone can be due to benign, transient disease, symptom complexes are more useful for predicting serious pathology (Thompson et al., 2007). In the UK, this has led to the ‘two week wait guidelines’ for suspected cancer (Department of Health, 2000). This means that patients with symptoms most predictive of colorectal cancer (Table 10.1) must be seen within 2 weeks from the date of referral.
Table 10.1 Criteria for urgent referral for suspected colorectal cancer under the two-week rule
| Sign, symptom or combination | Age threshold |
|---|---|
| Rectal bleeding with a change in bowel habit to looser stools and/or increased frequency of defecation persistent for 6 weeks | Over 40 years |
| A definite right-sided abdominal mass | All ages |
| A definite palpable rectal (not pelvic) mass | All ages |
| Change of bowel habit to looser stools and/or increased frequency of defecation, without rectal bleeding and persistent for 6 weeks | Over 60 years |
| Rectal bleeding persistently without anal symptoms | Over 60 years |
| Iron deficiency anemia without an obvious cause (Hb<11 g/dl in men or <10 g/dl in postmenopausal women) | No age criterion |
Rectal bleeding
Bleeding from the gastrointestinal tract can be overt or occult. With overt rectal bleeding, the blood is recognized and is usually noticed on defecation. If this is the case, the origin of the bleeding is usually in the left colon or distal transverse colon. If the bleeding is occult, the blood loss is not recognized in the stool and the patient presents with anemia.
Bright red rectal bleeding with anal symptoms
Rectal bleeding with anal symptoms without a change in bowel habit is the lowest predictor of colorectal cancer (Thompson et al., 2007). It usually suggests hemorrhoids (associated with mucus, skin tags or prolapsing lumps) or an anal fissure (associated with anal pain on defecation). Distal proctitis (inflammation of the very distal rectum) may also be a cause. The exception to this is anal cancer that may present with these symptoms but is often associated with a lump or ulcer in the anal canal
Investigation: no radiological investigation may be necessary. This diagnosis can usually be made in the outpatient clinic on rigid sigmoidoscopy and/or proctoscopy. In the case of a fissure, examination may not be possible and a painful per rectum (PR) examination may be diagnostic.
Bright red rectal bleeding without anal symptoms
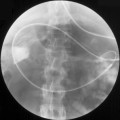
Investigation: radiological investigation may not be necessary for this symptom complex. It should be diagnosed on PR examination ± rigid sigmoidoscopy or proctoscopy. Flexible sigmoidoscopy would be appropriate in the over 40s to exclude malignancy. Should a stricture prevent the passage of the endoscope, a barium enema (Figure 10.1) or computed tomography (CT) should be considered.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


