Fig. 3.1 Echocardiography transducer. Schematic depiction. The transducer permits intercostal views. |
1-D (M-mode) echocardiography,
2-D echocardiography,
3-D echocardiography, and
Doppler echocardiography.
 Fig. 3.2 Principles of 1-D echocardiography. Schematic depiction. Parasternal view with recordings in A-mode, B-mode, and M-mode. Ao = aorta AoV = aortic valve LA = left atrium LV = left ventricle RV = right ventricle |
 Fig. 3.3 1-D echocardiography in M-mode. Schematic depiction. M-mode sweep along the parasternal long axis with a recording of typical movement patterns of the left and right ventricles and the mitral and aortic valves during the cardiac cycle. Fractional shortening can be determined as a measure of left ventricular global function based on the LV-EDD and LV-ESD parameters. A = A-wave (mitral valve movement during atrial contraction) AoV = aortic valve E = E-wave (mitral valve movement during diastole, known as early filling) ECG = electrocardiogram LV = left ventricle LV-EDD = left ventricular end diastolic diameter LV-ESD = left ventricular end systolic diameter LV-PW = left ventricular posterior wall MV = mitral valve RV = right ventricle RV-AW = right ventricular anterior wall RVOT = right ventricular outflow tract |
 Fig. 3.4 Typical transducer positions during TTE. Schematic depiction. By using the depicted views, the heart and adjacent vessels can generally be depicted well in pediatric patients during a TTE. For children, even the suprasternal view often allows an aortic isthmus to be visualized. |
Parasternal long axis of the left ventricle (▶Fig. 3.5): This view primarily allows left ventricular size and function to be evaluated. In addition, this view allows 2-D and color Doppler visualization of the presence of a VSD in the perimembranous and muscular portion of the septum.
Parasternal short axis of the left ventricle (after rotating the transducer 90° and shifting it accordingly)
with a depiction of the aortic and pulmonary valves (▶Fig. 3.6), the pulmonary arterial stem, possible abnormal vascular connections such as a coronary fistula, abnormal connection of the coronaries to the pulmonary arterial stem (Bland-White-Garland syndrome), and, above all, PDA.
with a depiction of the mitral valve, the papillary muscles, or the apex (▶Fig. 3.7). This sectional plane allows the size and function of the left ventricle and the mitral valve opening to be assessed.

Apical 4-chamber and 5-chamber views: These views can depict the LVOT and aortic valve (▶Fig. 3.8). Abnormal structures and functional abnormalities, such as turbulences or regurgitation via the aortic valve, can be visualized using color Doppler.
Apical left 2-chamber view and apical long axis (by rotating the transducer 90° and angulating it appropriately): These views can depict the LVOT (▶Fig. 3.9).
 Fig. 3.5 2-D echocardiography—parasternal long axis of the heart. Schematic depiction. Ao = aorta AoV = aortic valve LA = left atrium LV = left ventricle RV = right ventricle |
 Fig. 3.6 2-D echocardiography—parasternal short axis of the heart. Schematic depiction. This sectional plane allows the aortic and pulmonary valve views to be depicted. AoV = aortic valve LA = left atrium PA = pulmonary artery PV = pulmonary valve RA = right atrium RVOT = right ventricular outflow tract TV = tricuspid valve |
 Fig. 3.7 2-D echocardiography—parasternal short axis of the heart. Schematic depiction. The parasternal long axis (a) is depicted with the corresponding short-axis slices (b) that occur when the transducer is rotated 90°. The red lines indicate the corresponding transducer position. Ao = aorta AML = anterior mitral leaflet LA = left atrium LV = left ventricle MV = mitral valve PML = posterior mitral leaflet a Parasternal long axis. b Short axis slices. |
 Fig. 3.8 Apical 4-chamber and 5-chamber view. Schematic depiction. Ao = aorta AoV = aortic valve LA = left atrium LV = left ventricle MV = mitral valve RA = right atrium RV = right ventricle TV = tricuspid valve. a Four-chamber view. b Five-chamber view. |
 Fig. 3.9 Apical 2-chamber view and LVOT cross-section. Schematic depiction. From an apical view, by rotating the transducer 90° in the 4-chamber view (a, red line), the apical 2-chamber view (b) and the apical long axis or LVOT cross-section (c) can be acquired by rotating the transducer appropriately. Ao = aorta AoV = aortic valve LA = left atrium LV = left ventricle MV= mitral valve a Four-chamber view. b Apical 2-chamber view. c Apical long axis or LVOT cross-section. |

 Fig. 3.10 3-D echocardiography. 3-D reconstruction of the tricuspid valve (before surgical reconstruction) for an 11-year-old girl with Ebstein’s anomaly, a free-floating leaflet (blue arrow), and chordal rupture. |


 Fig. 3.11 3-D echocardiography. Ao = aorta AoV = aortic valve a LVOT reconstructed from a 3-D data set with a thickened aortic valve. b 5-chamber view with a central ascending aorta. c 3-D reconstruction of a unicuspid aortic valve (before surgical valve reconstruction) in a 15-year-old girl with a combined aortic vitium. |
 Fig. 3.12 3-D echocardiography. 3-D volume reconstruction of the right ventricle in a patient with surgically treated tetralogy of Fallot and a significantly enlarged right ventricle. a Long-axis planimetry of the right ventricle (2-chamber view). b Total volume of the enlarged right ventricle determined using planimetry. c Long-axis planimetry of the right ventricle (4-chamber view). d Short-axis planimetry of the right ventricle. |
 Fig. 3.13 3-D echocardiography. EDV = end diastolic volume EF = ejection fraction ESV = end systolic volume SDI = systolic dyssynchrony index SV = stroke volume a Real-time 3-D reconstruction of a male patient’s left ventricle after correcting his pulmonary atresia correction. The left ventricular volume is subdivided into 17 segments according to the AHA, and the decrease in volume is measured and recorded in the individual segments during systole within a single cardiac cycle. At 29.64%, the patient’s left ventricular ejection fraction is reduced significantly. b Segmental curves of a test subject’s homogeneous volume change. All of the curves demonstrate a largely synchronous course. c Dyssynchronous volume changes in a male patient a from which an SDI can be calculated, which appears to be closely associated with left ventricular function. In particular, septal segments 1, 6, 7, and 12 demonstrate significant asynchrony after correcting the patient’s pulmonary atresia. |
Continuous-wave Doppler (CW Doppler): CW Doppler records all flow velocities along the sonic ray. It possesses a large penetration depth and allows high flow velocities to be recorded and quantified. Unlike a PW Doppler, however, it cannot precisely localize the site with the highest flow velocity.
Pulsed-wave (PW) Doppler: PW Doppler allows flow velocities to be recorded only within a “measuring range,” in a sample volume (measured volume). It possesses less penetration depth than a CW Doppler. Unlike the CW Doppler, however, PW Doppler allows precise localization of the recorded flow velocity.
Color Doppler: This type of Doppler is represented primarily by color Doppler, and constitutes the most
common type of Doppler echocardiography. The median flow velocities determined using many measurement volumes (sample volumes) are depicted in a color-coded 2-D image. Color Doppler echocardiography delivers not just information about blood flow velocity, flow turbulence, and flow volume, but also information about the direction and quality of blood flow in real time. Thus, it can be used for orientation, qualitative assessment of the extent of valve insufficiency or stenosis, or assessment of shunt size in cases of ASD or VSD.
 Fig. 3.14 Flow ratios in vascular or valvular stenoses. Schematic depiction. Application of the Bernoulli equation to assess pressure gradients based on maximum flow velocity using Doppler sonography. |
Table 3.1 Graduation of the aortic valve stenosis in Doppler ultrasound.4 | |||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||



Table 3.2 Graduation of aortic valve insufficiency measured via Doppler.4 | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||
 Fig. 3.15 TEE. Depiction of an ASD. LA = left atrium RA = right atrium RV = right ventricle a Schematic depiction of a TEE being performed and the most clearly visualized cardiac structures. b Large ASD depicted using TEE, with a significant left-right shunt (arrow) in a male patient with a limited transthoracic acoustic window. |
Assessing atrial structures (e.g., clots, tumors, intraatrial septal defects, valve morphology and function, changes in valves in the sense of endocarditis vegetation)
Assessing LVOT morphology
Assessing the aortic valves (unicuspid, bicuspid, or tricuspid aortic valves) and their function
Assessing the morphology and size of the ascending aorta (e.g., aortic dissection)

 Fig. 3.16 TEE. Depiction of an ASD. The interatrial septum can be clearly depicted via TEE. Multiplanar depiction of the septal defect (a–c, arrows) from various angles (0-180°; three angles are shown as an example [angular display listed top right in green]) allowing the size, extent, and shape of a defect to be visualized with precision before an interventional closure. LA = left atrium RA = right atrium a 37° angle. b 75° angle. c 168° angle. |
Parasternal (▶Fig. 3.4): long and short axis
Apical: 2-chamber and 4-chamber view, long axis
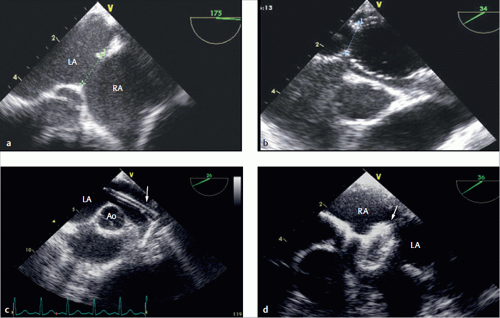 Fig. 3.17 Therapeutic closure of intraatrial communication during a TEE exam. Ao = aorta LA = left atrium RA = right atrium a Thorough measurement of the defect’s native size. b A guide wire is subsequently placed in the left pulmonary vein via a catheter. c The sizing balloon is then introduced into the defect via the wire and inflated carefully. This allows precise assessment of the defect’s size. An appropriate catheter (arrow) is then introduced into the left atrium using the same guide wire. d The appropriate AmplatzerTM septal occluder is placed using the catheter during TEE monitoring, and only the left atrial disc is deployed (arrow). |
 Fig 3.17 (Continued) Therapeutic closure of intraatrial communication during a TEE exam. Ao = aorta LA = left atrium RA = right atrium e The left atrial disk is then adapted carefully to the intraatrial septum or defect. f The right atrial disc is carefully released by slowly withdrawing the wire, thereby closing the defect. g During TEE monitoring, a stress test is performed by pulling and pushing on the probe before the occluder is detached from the wire. h The placement and position of the occluder are examined and monitored from different angles while the occluder is still attached to the wire. |
 Fig. 3.18 Echocardiographic wall motion analysis. Schematic depiction. The blue contour indicates the end diastolic and the red contour, the end systolic border of the left ventricle in a 4-chamber view in a healthy patient and in the presence of various pathologies. |
 Fig. 3.19 American Society of Echocardiography’s modified 18-segment model. Schematic depiction. The numbers indicate the 18 segments. |
 Fig. 3.20 Atropine administration. Schematic depiction. Stress protocols with dipyridamole and dobutamine. The highlighted minute labels indicate the point of recording. BW = body weight |
regional myocardial function or dyssynchronous contractile behavior in the left and right ventricles. In the example case of a boy with aortic valve stenosis and myocardial hypertrophy of the interventricular septum, a significant change in the deformation was visible before and after being subjected to pharmacological stress conditions (▶Fig. 3.21). The new methods of 2-D strain or speckle tracking should also be considered when assessing myocardial function under stress conditions.
 Fig. 3.21 Quantitative analyses of regional myocardial velocity and deformation under stress conditions. a Deformation (strain) in the interventricular septum of a boy with pressure overload in the left ventricle due to an aortic valve stenosis. b Clear visibility of post-systolic contraction as an expression of possible myocardial fibrosis after a pharmacological stress test using Alupent. |
high-amplitude myocardial signals are recorded, while high-velocity, low-amplitude blood flow signals are filtered out. Both PW and color Doppler are used. Myocardial tissue Doppler has not yet established itself in routine diagnostics. A combined approach using color Doppler to assess myocardial wall motion during stress, however, appears useful. Earlier approaches hope for improved characterization of diastolic wall motion abnormalities,26 meaning also in cases of complex congenital heart defects.27


(along the ultrasonic beam) at a defined distance from one another by the original distance between those two points. This allows us to calculate the deformation rate (strain rate):
 Fig. 3.22 Tissue Doppler ECG. Schematic depiction. Recording of wall velocities and deformations at defined points. Special filters are applied in order to suppress signals from the blood and record only signals from the myocardial wall. |
 Fig. 3.23 Tissue Doppler ECG. Example schematic depiction of wall velocities and time intervals derived from a tissue Doppler during a cardiac cycle. In addition to determining systolic, early diastolic, and late diastolic velocity, it is also possible to calculate important time intervals, such as isovolumetric contraction and relaxation time. This allows the Tei index to be calculated as a parameter of the global function using the following formula: Tei index = (A – B)/B. AoV = aortic valve AT = late diastolic velocity ET = early diastolic velocity ICT = isovolumetric contraction time IRT = isovolumetric relaxation time SystT = systolic velocity |
 Fig. 3.24 Myocardial strain or deformation. Schematic depiction. The longitudinal, radial, and circumferential myocardial wall deformations can be determined using special software and a more precise configuration for data acquisition. |


point travelled during this time. Thus, velocity can be calculated using displacement within the sequence of images relative to time. Strain and strain rate can both be determined based on velocity (▶Fig. 3.26).
 Fig. 3.25 Speckle tracking or 2-D strain. Schematic depiction. Speckle tracking does not use the Doppler principle to calculate myocardial velocity. |
 Fig. 3.26 Speckle tracking. The myocardial walls can be recorded semi-automatically using this new method. Wall velocities, deformations, and deformation rates can be calculated in the recorded region using special software. A = atrial peak AVC = aortic valve closure E = early filling peak S = systolic peak a Determining wall velocity. b Determining deformations. c Determining deformation rates. |
multiple-row detector systems, and DSCT (dual source CT) were the primary contributors to cardiac CT as it is performed today.
 Fig. 3.27 DSCT. CT with two complete measurement systems.31 a Schematic depiction of the principle of the scanner. b Photo of a clinical installation. |

systems allows the effective scan time to be cut in half. At minimum, a scan range of 180° plus fan angle is needed for image reconstruction. DSCT scans can provide this information after only a 90° rotation. Furthermore, double X-ray power is available. This is of great importance particularly to images with short effective scan times, since this exposes the patient to the required radiation dosage for the shortest possible period of time.
Table 3.3 Features of modern high-performance CT scanners. | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 Fig. 3.28 DSCT image of a heart. One-year-old child. Measurement parameter: 75 ms effective slice scan time, 0.26 s overall scan time, 1.1 mSv effective dose. a Axial reconstruction. b Coronal reconstruction. c Sagittal reconstruction. (Courtesy of Prof. Dr. M. Lell, Erlangen.) |

 Fig. 3.29 DSCT image of a heart. 3-D dose distributions calculated using the Monte Carlo approach for the CT exam shown in ▶Fig. 3.28. a Axial. b Coronal. c Sagittal. |




exam doses. The medical authority will, however, first attempt to consult with examiners to reduce median dose values.

 Fig. 3.30 Dose calculation for various age groups.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|