Massive bleed from a Meckel diverticulum: uptake of 99mTc pertechnetate if ectopic gastric mucosa is present. Hemolytic-uremic syndrome, ulceration, IID, tumors, angiodysplasia, intussesception.
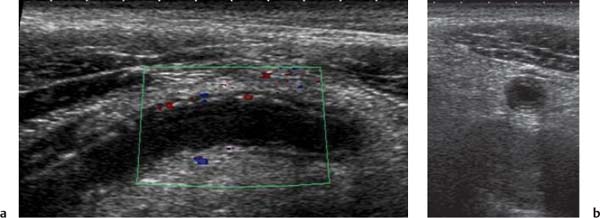
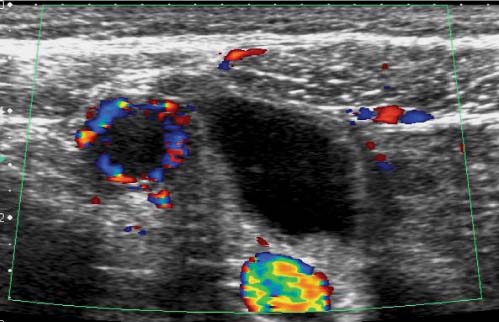
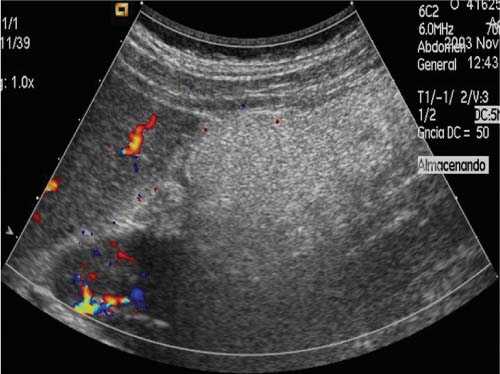
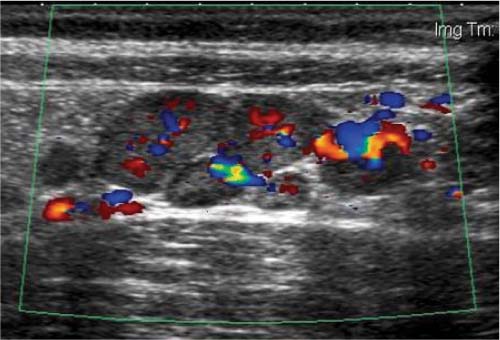
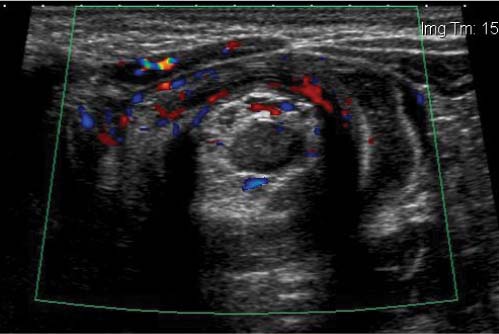
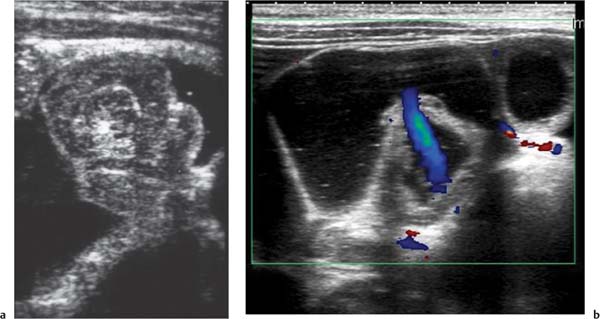
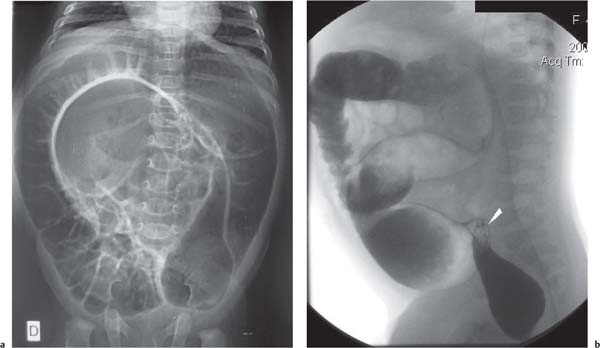
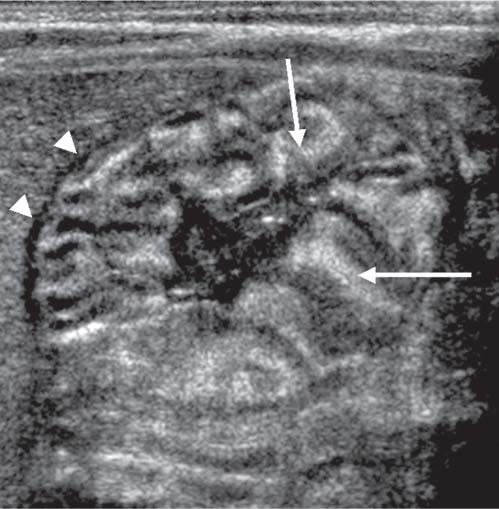
Fig. 2.138a, b Acute appendicitis. RLQ US, longitudinal (a) and axial (b) views, shows a dilated obstructed appendix with a thin-rings pattern: the normal bowel wall layers are patent, unless their thickness is decreased and the lumen is occupied by purulent anechoic content. In axial view, there is an increased sound transmission pointing to the fluid nature of the content. The hyperechoic mesenteric fat is enlarged. The Doppler signal (longitudinal view) is increased in appendix wall.Fig. 2.139 Acute appendicitis. Transverse Doppler US image of RLQ: An inflamed hypervascularized appendix is depicted. Note the difference in size and vascularization with the adjacent fluid-filled ileum.Fig. 2.140 Omental segmental infarction. Sagittal Doppler US scan in mesogastric area: A hyperechoic avascular thickened omen-tum is seen beside the liver and kidney. The inflamed fat-containing omentum progressively attenuates the US beam.Fig. 2.141 Mesenteric adenitis. Transverse Doppler US image in mesogastric area: There are several slightly increased in size (> 6 mm) mesenteric lymph nodes with patent vascularization. This is a nonspecific finding, and other causes of acute abdomen must be ruled out. In this case, the appendix (not shown) was normal.Fig. 2.142 Intussusception. US axial image of an intussesception depicted at the subhepatic region. There is a thick hypoechoic outer “doughnut” with a crescent-shaped hyperechoic mesentery inside, eccentrically surrounding a hypoechoic central limb of the intussusceptum. This is the “crescent-in-doughnut” sign.Fig. 2.143 Intussusception. US longitudinal image of an intussesception. There are several alternating bands that represent the hypoechoic intussesception and the hyperechoic mesentery. This is the “sandwich” sign.Fig. 2.144 Intussusception. US axial image of an intussesception in the subhepatic region shows the double “crescent-in-doughnut” sign. There is an additional anechoic crescent inside the doughnut formed by trapped ascites located opposite to the mesenteric hyperechoic crescent. The presence of ascites is related with bowel ischemia and low reducibility rates. G GallbladderFig. 2.145 Intussusception. Doppler US axial image of an intussesception showing blood flow in the peripheral doughnut and in the central mesentery. The presence of blood flow is a good prognostic sign of reducibility.Fig. 2.146a, b Intussusception reduction. (a) During the hydrostatic echo-guided enema, the intussesception is seen partially reduced at the level of the ileocecal valve. (b) After intussesception reduction, the valve is seen open and with fluid passage through terminal ileum (blue color in the Doppler image).Fig. 2.147 Ileoileocolic intussusception. Longitudinal US during hydrostatic echo-guided enema shows a complex polylobulated ileoileo-colic intussesception with fluid trapped inside attempting to pass through the valve. In this case, the reduction was not possible.Fig. 2.148a, b Sigmoid volvulus. (a) Plain abdominal film shows a distal colonic obstruction with the “coffee-bean sign,” which is formed by twisted sigmoid colon and distended proximal colonic loops. (b) Contrast enema delineates the areas of sigmoid narrowing after devolvulation (arrowhead).
The Acute Abdomen in the Neonatal Period
Table 2.69 Acute abdomen in the neonatal period
Diagnosis
Findings
Comments
Gastric outlet obstruction
Plain X-ray: “single-bubble” image. When a single bubble is observed, most patients are taken directly to surgery.
Causes: antral or pyloric atresia, congenital peritoneal bands, annular pancreas.
US: mucosal thickening often with polypoid or lobular appearance (DD with the muscular thickening observed in hypertrophic pyloric stenosis).
After administration of prostaglandin E to infants with ductus-dependent congenital heart disease. The stenosis is produced by central foveolar hyperplasia.
Complete duodenal obstruction
More frequent than gastric obstruction.
Plain radiograph: “double-bubble” image. Rarely require further radiologic investigation.
Causes: duodenal atresia, annular pancreas, and midgut volvulus. Less frequently secondary to duodenal web, Ladd band, or preduodenal portal vein.
Incomplete duodenal obstruction
Plain X-ray: distention of the stomach and duodenum with a diminished air in the small bowel. DD with HPS by US.
UGI series: to differentiate midgut volvulus from a web or stenosis.
US: to rule out extraluminal causes (duplication cyst).
Contrast enema: the critical DD finding on the contrast enema of a neonate with low obstruction is the presence or absence of a microcolon.
Occurring in the distal ileum or colon.
Symptoms: vomiting, abdominal distention, and failure to pass meconium.
Causes: ileal atresia, meconium ileus, colonic atresia, Hirschsprung disease, and functional immaturity of the colon.
Meconium peritonitis
Plain X-ray: linear or punctate calcifications over the serosal surfaces of the abdominal viscera. Decubitus X-ray to determine the presence of free air with a persistent perforation is essential.
US: especially indicated in the presence of a relatively airless abdomen.
In-utero perforation of the fetal GI tract during the last 6 mo of pregnancy. May occur with meconium ileus but may occur with any type of obstruction and in utero perforation.
Anorectal malformations
Anorectal malformations are almost always evident on physical examination.
Pneumoperitoneum of GI origin
Left lateral decubitus radiograph most reliable.
It is usually the result of a hollow viscus perforation.
In healthy neonates, is usually iatrogenic. Other causes: necrotizing enterocolitis, atresias, meconium ileus, congenital megacolon.
Pneumoperitoneum of pulmonary origin
Air passes to the abdomen through the normal diaphragmatic foramina. There is no perforation of the GI tract in these cases.
Necrotizing enterocolitis
Abdominal X-ray: linear or cystic pneumatosis intestinalis (submucosal or subserosal air).
Portal vein gas: finely branching radiolucencies extending from the porta hepatis to the periphery of the liver. On US: bright, shifting echogenic foci within the portal vein.
Pathophysiology: ischemia, decreased mucus production, diminished immune response of the premature infants.
Massive ascites
US, abdominal radiograph to exclude complications, free air, or calcifications.
In congenital hydrops, urinary tract perforation (e.g., urethral valves), or GI perforation.
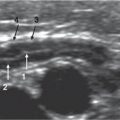
Fig. 2.149 Pyloric hyperthropy. A neonate with ductus-dependent congenital heart disease treated with prostaglandin E to keep the ductus open. Axial US scan through the gastric antrum reveals markedly hypertrophic mucosal folds (arrows) with an undulating appearance. The thickness of the muscular layer is normal (arrowheads).
Further Reading
Baltazhar EJ. Complications of acute pancreatitis: clinical and CT evaluation. Radiol Clin North Am 2002;40:1211–1229Benya EC. Pancreas and biliary system: imaging of developmental anomalies and diseases unique to children. Radiol Clin North Am 2002;40:1355–1362Berrocal T, del Pozo G. Imaging in pediatric gastrointestinal emergencies. In: Devos AS, Blickman H, ed. Radiological imaging of the digestive tract in infants and children. Berlin: Springer Verlag, 2008:1–78Berrocal T, Lamas M, Gutieérrez J, et al. Congenital anomalies of the small intestine, colon and rectum. Radiographics 1999;19:1219–1236Berrocal T, Parrón M, Alvarez-Luque A, Prieto C, Santamaría ML. Pediatric liver transplantation: a pictorial essay of early and late complications. Radiographics 2006;26:1187–1209Berrocal T, Torres I, Gutiérrez J, Prieto C, del Hoyo ML, Lamas M. Congenital anomalies of the upper gastrointestinal tract. Radiographics 1999;19:855–872Boudiaf M, Jaff A, Soyer P, Bouhnik Y, Hamzi L, Rymer R. Small bowel diseases: prospective evaluation of multi-detector row helical CT enteroclysis in 107 consecutive patients. Radiology 2004;233:338–344Callahan MJ, Rodriguez DP, Taylor GA. CT of appendicitis in children. Radiology 2002;224(2):325–332Carty HM. Paediatric emergencies: non-traumatic abdominal emergencies. Eur Radiol 2002;12(12):2835–2848Cazier PR, Sponaugle DW. “Starry sky” liver with fasting: variation in glycogen stores? J Ultrasound Med 1996;15:405–407Christison-Lagay ER, Burrows PE, Alomari A, et al. Hepatic hemangiomas: subtype classification and development of a clinical practice algorithm and registry. J Pediatr Surg 2007;42:62–68Daneman A, Navarro O. Intussusception. Part 2: an update on the evolution of management. Pediatr Radiol 2004;34:97–108del-Pozo G, Albillos JC, Tejedor D. Intussusception: US findings with pathologic correlation—the crescent-in-doughnut sign. Radiology 1996;199:688–692del-Pozo G, Albillos JC, Tejedor D, et al. Intussusception in children: current concepts in diagnosis and enema reduction. Radiographics 1999;19:299–319del-Pozo G, González-Spinola J, Gómez-Ansón B, et al. Intussusception: trapped peritoneal fluid detected with US-relationship to reducibility and ischemia. Radiology 1996;201:379–386del-Pozo G, Miralles M, Sánchez L, et al. Apendicitis aguda en la infancia. Hallazgos ecográficos frecuentes e infrecuentes. Radiología 1994;36:411–424Furukawa A, Saotome T, Yamasaki M, et al. Cross-sectional imaging in Crohn disease. Radiographics 2004;24:689–702Gonzalez-Spinola J, del Pozo G, Tejedor D, et al. Intussusception: the accuracy of ultrasound-guided saline enema and the usefulness of a delayed attempt at reduction. J Pediatr Surg 1999;34: 1016–1020Grazioli L, Federle MP, Brancatelli G, Ichikawa T, Olivetti L, Blachar A. Hepatic adenomas: imaging and pathologic findings. Radiographics 2001;21:877–892Ha A, Levine M, Rubesin S, Laufer I, Herlinger H. Radiographic examination of the small bowel: survive of practice patterns in the United States. Radiology 2004;231:407–412.Hammond N, Miller FH, Sica GT, Gore RM. Imaging of cystic diseases of the pancreas. Radiol Clin North Am 2002;40:1243–1263Helmberger TK, Ros PR, Mergo PJ, Tomczak R, Reiser MR. Pediatric liver neoplasms: a radiologic-pathologic correlation. Eur Radiol 1999;9:1339–1347Hilmes MA, Strouse PJ. The pediatric spleen. Semin Ultrasound CT MR 2007;28(1):3–11Jamieson D, Shipman P, Israel D, Jacobson K. Comparison of multidetector CT and barium studies of the small bowel: inflammatory bowel disease in children. AJR Am J Roentgenol 2003;180:1211–1216Jamieson D, Stringer DA. Small bowel. In: Stringer DA, Babin PS, ed. Pediatric gastrointestinal imaging and interventional. Hamilton, Ontario, Canada: BC Decker, 2000:396–400Kaiser S, Frenckner B, Jorulf HK. Suspected appendicitis in children: US and CT—a prospective randomized study. Radiology 2002;223(3): 633–638Kehagias D, Moulopoulos L, Antoniou A, et al. Focal nodular hyperplasia: imaging findings. Eur Radiol 2001;11:202–212Keyzer C, Tack D, de Maertelaer V, Bohy P, Gevenois PA, Van Gansbeke D. Acute appendicitis: comparison of low-dose and standard-dose unenhanced multi-detector row CT. Radiology 2004;232(1): 164–172Kimmey MB, Martin RW, Haggitt RC, Wang KY, Franklin DW, Silverstein FE. Histologic correlates of gastrointestinal ultrasound images. Gastroenterology 1989;96:433–441King LF, Scurr ED, Natajaran M, Williams SGF, Westaby D, Healy JC. Hepatobiliary and pancreatic manifestations of cystic fibrosis: MR imaging appearances. Radiographics 2000;20:767–777Kuhn JP, Slovis TL, Haller JO, ed. Caffey’s pediatric diagnostic imaging. Philadelphia, PA: Elsevier Inc., 2004Ly JN, Miller FH. MR imaging of the pancreas: a practical approach. Radiol Clin North Am 2002;40:1289–1307Marincek B. Nontraumatic abdominal emergencies: acute abdominal pain: diagnostic strategies. Eur Radiol 2002;12:2136–2150Metreweli C, So NM, Chu WC, Lam WW. Magnetic resonance cholangiography in children. Br J Radiol 2004;77:1059–1064Norton KI, Glass RB, Kogan D, Lee JS, Emre S, Shneider BL. MR cholangiography in the evaluation of neonatal cholestasis: initial results. Radiology 2002;222:687–691Pariente D. The liver, biliary tract and spleen. In: Carty H, Brunelle F, Shaw D, Kendall B, ed. Imaging children. London, England: Churchill Livingstone, 1994:485–560Park NH, Park SI, Park CS, et al. Ultrasonographic findings of small bowel intussusception, focusing on differentiation from ileocolic intussusception. Br J Radiol 2007;30:798–802Paterson A, Frush DP, Donnelly LF, Foss JN, O’Hara SM, Bisset GS 3rd. A pattern-oriented approach to splenic imaging in infants and children. Radiographics 1999;19(6):1465–1485Puylaert JB. Right-sided segmental infarction of the omentum: clinical, US, and CT findings. Radiology 1992;185:169–172Puylaert JB. Ultrasonography of the acute abdomen: gastrointestinal conditions. Radiol Clin North Am 2003;41(6):1227–1242Puylaert JB, Vermeijden RJ, Van der Werf SDJ, Doornbos L, Koumans RK. Incidence and sonographic diagnosis of bacterial ileocaecitis masquerading as appendicitis. Lancet 1989;2:84–86Remer EM, Baker ME. Imaging of chronic pancreatitis. Radiol Clin North Am 2002;40:1229–1243Robertson F, Leander P, Ekberg O. Radiology of the spleen. Eur Radiol 2001;11(1):80–95Roebuck DJ, Olsen Ø, Pariente D. Radiological staging in children with hepatoblastoma. Pediatr Radiol 2006;36:176–182Rubesin S. Simplified approach to differential diagnosis of small bowel abnormalities. Radiol Clin North Am 2003;41:343–364Scatarige JC, Horton KM, Sheth S, Fishman EK. Pancreatic parenchymal metastases: observations on helical CT. AJR Am J Roentgenol 2001;176:695–699Strouse P. Disorders of intestinal rotation and fixation (“malrotation”). Pediatr Radiol 2004;34:837–851Taylor GA. Suspected appendicitis in children: in search of the single best diagnostic test. Radiology 2004;231(2):293–295Valls C, Iannacconne R, Alba E, et al. Fat in the liver: diagnosis and characterization. Eur Radiol 2006;16:2292–2308Ziegler MM. The diagnosis of appendicitis: an evolving paradigm. Pediatrics 2004;113:130–132
Only gold members can continue reading. Log In or Register to continue