The spleen is a wedge-shaped organ that is convex supero-laterally and concave inferomedially with a vascular hilum. It can be affected either by primary pathologic process or by multiorgan or systemic disease. Its histology varies with age, with little white pulp in the neonate, which increases with age.
Table 2.22 Normal imaging
Diagnosis
Findings
Comments
US
Homogeneous, slightly hyperechoic than normal kidney.
With high-frequency transducers, a granular pattern can be seen in children aged 1 to 5 y.
CT
Unenhanced CT: Homogeneous. With contrast, irregular, bizarre patterns of enhancement that disappear in portal phase (> 70 s).
MR
Neonate: Hypointense on T2 and hyperintense (to liver) on T1. From 1 year of age, adult pattern: hyperintense on T2 and hypointense on T1. Irregular pattern of enhancement.
Nuclear medicine (NM)
99mTc-labeled heat-damaged red cells are only taken up by the spleen.
Useful if a normal spleen is not detected by other imaging methods.
Table 2.23 Changes in position and shape
Diagnosis
Findings
Comments
Notches, clefts, and lobulations
Lobules are located near the hilum or extending anterior to the upper pole of the kidney. Clefts are sharp, located in the superior border, and sometimes 2–3 cm deep.
Normal in fetal period, usually disappear, but may be present into adult life.
Wandering spleen: migration from its original position to a more caudal location because of laxity or lack of ligament fixation.
Wandering spleen is more common in females. It usually presents as an abdominal mass or as an acute abdomen due to torsion of the vascular pedicle with possible infarction.
Common anomaly (> 30%). Usually < 15 mm and located near the hilum, but can be multiple and in other locations. Same pattern that normal spleen.
Clinically insignificant. Increase in size after splenectomy.
Polysplenia syndrome (levoisomerism)
Multiple discrete spleens, right- or left-sided (at the same side of the stomach). Cardiac anomalies. Liver centrally located. No intrahepatic IVC, with azygous continuation. Mirror location of GI organs.
Wide range of abdominal anomalies. Most patients have severe cardiac anomalies, but 5%–10% reach adulthood without symptoms. More frequent in females.
Absence of spleen. Severe congenital heart disease. Liver and gallbladder in midline. IVC and aorta lie on the same side of column. Short pancreas. Midgut malrotation.
Most die in the first year. Male predominance.
Vascular shunts
Splenogonadal, splenorenal, splenohepatic.
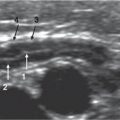
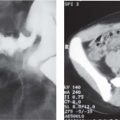
Fig. 2.39 Situs inversus. Transverse US through epigastrium shows a left-located liver and gallbladder and a right-sided air-distended stomach (ST).Fig. 2.40 Accessory spleen. Longitudinal US shows an isoechoic splenic parenchyma nodule (arrowhead) near the splenic hilum, representing accessory tissue.Fig. 2.41 Asplenia syndrome. Plain film in a neonate showing the central position of liver.
Table 2.24 Splenomegaly
Diagnosis
Findings
Comments
Infection, sepsis
Usually homogeneous splenomegaly.
Many causative organisms: Bacterial, viral, protozoal, fungal. Some of them produce isolated splenomegaly: Ebstein-Barr virus, malaria, histoplasma, mycobacterium.
Portal hypertension
Often due to extrahepatic portal vein thrombosis:
Doppler US with absent or reversed flow or with cavernomatous transformation. Splenomegaly with heterogeneous hepatomegaly with lobulated margins.
Common causes: liver disease, umbilical vein catheterization, tumor, dehydration, omphalitis, hypercoagulability states.
Multiple focal masses. Lymphoma can invade the capsule. Lymphadenopathy in hilum and retroperitoneum can be seen.
Look for other manifestations of disease.
Gaucher, Niemann-Pick disorders
Multiple nodules. On MRI, T1 signal is lower than for normal spleen.
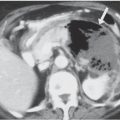
Fig. 2.43Salmonella abscess. Longitudinal US in a 17-year-old boy with Salmonella infection and fever. A solitary abscess (between arrowheads) was found in splenic parenchyma.Fig. 2.44Candida abscess. In a neutropenic 5-year-old girl treated for neuroblastoma, transverse US shows multiple fungal abscess cavities.Fig. 2.45 Pyogenic abscess. Contrast-enhanced CT in a 15-year-old boy with a pyogenic abscess treated with percutaneous drainage.Fig. 2.46 Non-Hodgkin lymphoma. Longitudinal US shows multiple heterogeneous solid nodules.Fig. 2.47 Metastasis. Contrast-enhanced CT shows a discrete splenic mass (between arrowheads) representing metastasis from renal sarcoma.