A large number of GI diseases can manifest as right lower quadrant (RLQ) acute pain, and some of them are potentially surgical. Knowledge of ileocecal region pathology is crucial in order to achieve an adequate differential diagnosis.
Table 2.52 Diseases of distal ileum, cecum, and appendix
Symmetrical thickness due to mucosal lymphoid hyperplasia of the terminal ileum (Peyer patches). Cobblestone appearance or adenitis. Colonic involvement associated.
Clinically simulates appendicitis and radiologically simulates nonstenotic Crohn disease. Caused by Yersinia enterocolitica or Campylobacter jejuni (Gram-negative rod), Salmonella typhosa infection (typhoid fever) with splenomegaly, anisakiasis.
Mimics Crohn disease: more localized in the ileocecal region. Commonly, ileitis extends to the colon (coned cecum).
Acute agranulocytic cecal enteritis: typhlitis
Dilatation. Marked thickening of the bowel wall with submucosal (edema and hemorrhage) predominance can be observed. Thumbprinting. Risk of perforation.
Commonly in immunosuppressed leukemic therapy (second week). Necrotizing enteritis of the right colon and ileocecal region. Nonsurgical appendicitis.
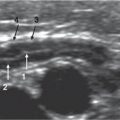
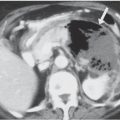
Fig. 2.102 Nodular lymphoid hyperplasia in a patient with hyperimmunoglobulin E syndrome. (a) Multiple discrete, round nodules throughout the small bowel are seen. (b) Irregular mucosal fold thickening with an added pattern of fine nodulation is noted.Fig. 2.103 Nodular lymphoid hyperplasia of ileum. Longitudinal US scan of terminal ileum is depicted between the abdominal wall muscles and psoas. The wall is slightly thickened with hypoechoic mucosal predominance. The serrated lumen is delineated by the hyper-echoic mucosal surface.Fig. 2.104a, b Ileocecitis due to Yersinia . (a) Ileocecal area. (b) Ascending colon: US shows parietal thickening of the ileum, cecum, and ileocecal valve. The ileum predominates the hypoechoic follicular mucosal hyperplasia, although in the cecum the hyperechoic submucosal layer is dominant. In the ascending colon, an accordion appearance is seen.Fig. 2.105 Yersiniosis. Compression spot radiograph of a small-bowel examination in a patient with a self-limited diarrheal illness and RLQ pain shows fold thickening with nodulation and ulcers in the distal ileum. Differentiation from Crohn disease is impossible. Resolution of the disease with antibiotic treatment provided a definitive diagnosis.Fig. 2.106a, b Tuberculosis. (a) Compression spot radiograph of a small-bowel examination. Note the nodular and edematous appearance of the distal ileum. Ulceration (arrows) and medial cecal affectation are present. (b) Contrast-enhanced CT scan shows bowel wall thickening in the distal ileum (arrow) with diffuse infiltration in the regional mesentery.
Only gold members can continue reading. Log In or Register to continue