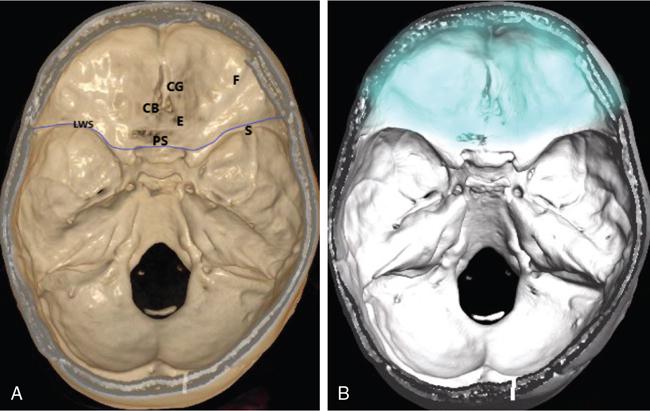
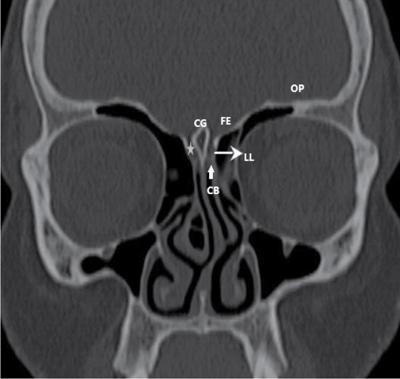
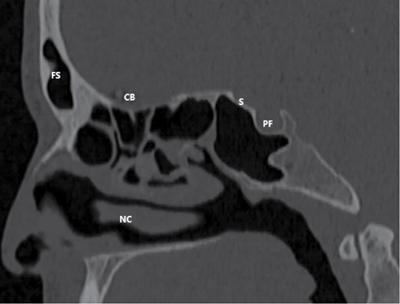
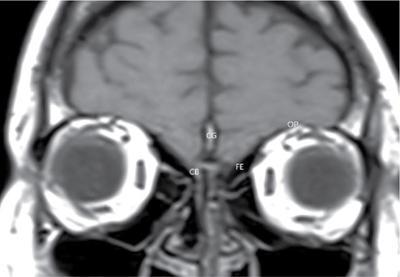
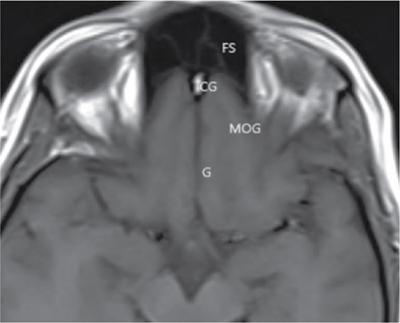
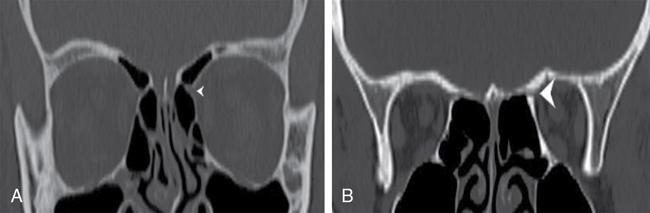
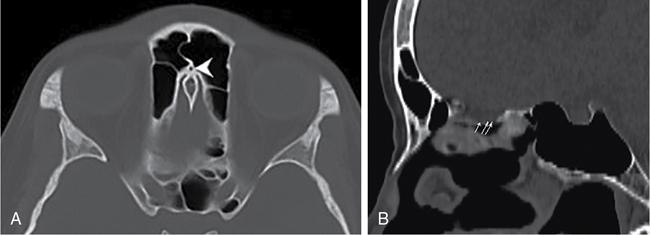
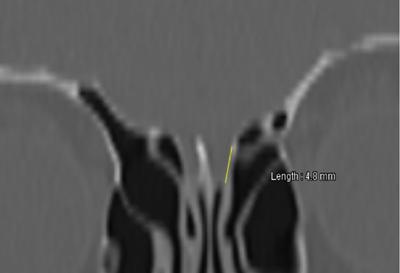
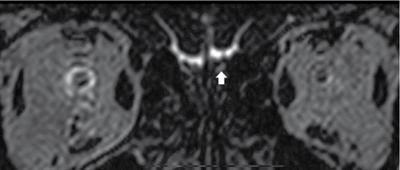
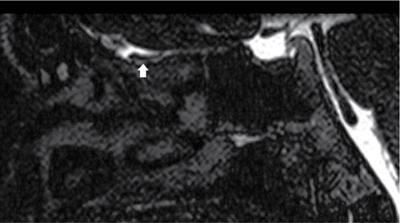
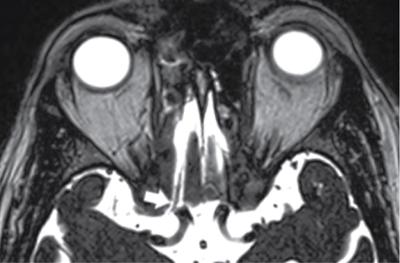
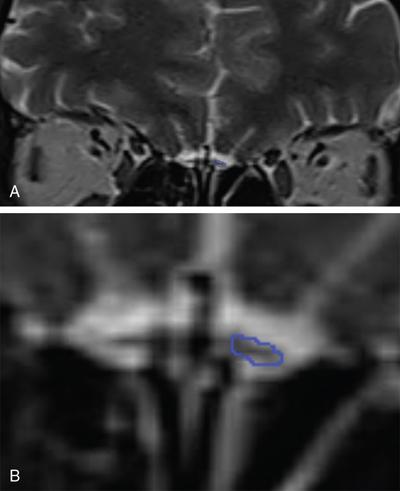
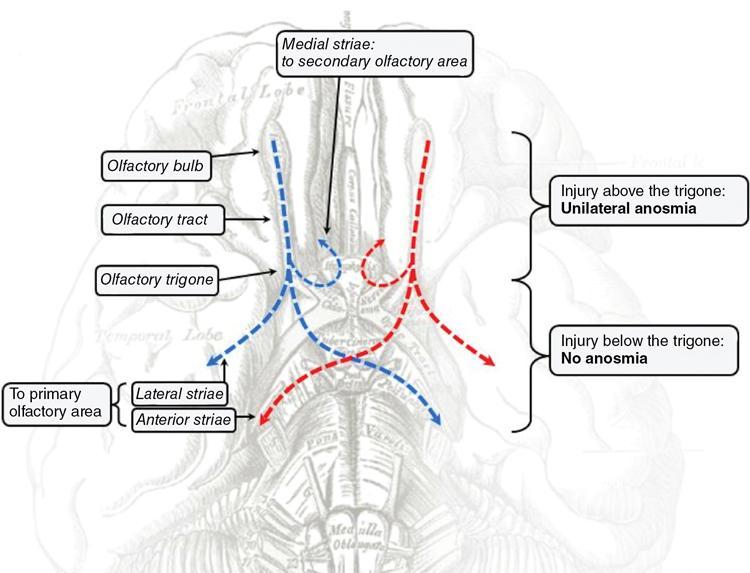
Subarekha TB, S. Rajakokila, R.S. Aarathhi Dhevi Vikramavel The anterior skull base is the bottom of the anterior skull, separating the anterior cranial fossa from the paranasal sinuses and the orbits. The anterior skull base (Figs 3.26.1–3.26.6) is formed by three bones – frontal, ethmoid and sphenoid. Anterior margin is formed by the frontal bone and the frontal sinuses. Central aspect of the anterior skull base is formed by the cribriform plate of the ethmoid bone separated by crista galli in the midline. The crista galli is a bony ridge and is the landmark for the anterior attachment of the falx cerebri. The cribriform plate (Fig. 3.26.3) is a thin plate of bone with multiple perforations in it, like a sieve, which transmits the olfactory rootlets from the nasal cavity to the subarachnoid space. The cribriform plate is shouldered by the lateral lamella on either side. The lateral lamella (Fig. 3.26.3) is continuous as the fovea ethmoidalis, forming the ethmoid roof, which further continues laterally as the orbital plate of the frontal bone. Orbital plate of the frontal bone also forms the roof of the orbit. Posterior margin of the anterior skull base is formed by the planum sphenoidale and lesser wing of sphenoid (Fig. 3.26.2). Anterior ethmoidal foramen marks the junction of the anterior and posterior ethmoidal sinuses on imaging. Skull base originates from the cartilaginous precursors. Ossification is from posterior to anterior and is constant in the first 2 years of life. By 6 months of age, roof of nasal cavity appears well ossified. By first year, crista galli appears well ossified on CT. By one and half years of life, ethmoid ascends above the cribriform plate forming the fovea ethmoidalis and after 24 months, anterior skull base is completely formed. Foramen cecum ossifies around 5 years of age. The depth of the olfactory fossa is determined by the height of the lateral lamella of the cribriform plate, which can be classified into three categories: Assessment of the olfactory fossa depth is significant in planning surgeries of the nose and orbit. The type 3 exposes more of the very thin cribriform plate to potential damage from trauma, tumour erosion, CSF erosion (in benign intracranial hypertension) and local nasal surgery/orbital decompression (Fig. 3.26.9). Olfaction is the oldest of the senses and hence is carried out by the first of the 12 pairs of cranial nerves, the olfactory nerve. The olfactory nerve is a peculiar cranial nerve and has only two neurons but transmits a complex sense of smell which is also linked to memory, taste and emotions. It is located superficially and somehow precariously in the olfactory fossa where it is almost openly in contact with the external world and hence easily affected by trauma and other pathologies. The posterosuperior aspect of the nasal cavity and the lateral aspects of the nasal septum close to the nasal vault are lined by olfactory epithelium. This epithelium lines approximately 2 sq cm area of the nasal vault. The first order axons of the olfactory nerves are the basal projections of the olfactory epithelium. These are unmyelinated axons which are the olfactory filia traverse the cribriform plate of the ethmoid bone through the multiple openings. These enter the cranial cavity penetrating the meninges and reach the subarachnoid space, where they enter the ventral surface of the olfactory bulb (Figs 3.26.10 and 3.26.11). The olfactory bulb is the tuft of glomeruli formed by the olfactory filia/nervelets. The olfactory bulb (Figs 3.26.10 and 3.26.11) is seen at undersurface of the anteromedial frontal lobe in the olfactory fossa and continues dorsally as the olfactory tract (Fig. 3.26.12). The olfactory tract, like the optic nerve, is a projection of the brain, developing as an outpouching of the ventral surface of telencephalon, rostral to the lamina terminalis. The olfactory bulb and olfactory tract are together known as the olfactory nerve (Fig. 3.26.13). The dorsal portion of the olfactory tract forms the olfactory trigone from which there are three main central connections. The central connections are described as follows. Lateral olfactory striae: Majority of the olfactory nerve tracts course over insula to reach the prepiriform cortex (anterior to uncus) and amygdala. They give collaterals to the subfrontal and frontal olfactory cortex. Further projections/collaterals to the subthalamic nuclei, thalamus and stria medullaris. These are phylogenetically newer. Medial olfactory striae: Major part of the fibres is seen terminating the paraolfactory area of Broca, which is the medial aspect of the subcallosal gyrus. Some of the fibres of the olfactory tract reach the subcallosal gyrus and anterior perforating substance. Some fibres cross in the anterior commissure and reach the opposite olfactory tract. Intermediate olfactory striae: Intermediate striae terminate in the anterior perforated substance. Intermediate olfactory area contains the anterior olfactory nucleus and the nucleus of the diagonal band. These are the fibres from the basal olfactory region, periamygdaloid area and septal nuclei. Majority of the fibres reach the autonomic area in the reticular formation, salivatory nucleus and dorsal vagal nucleus. Some of the fibres from the medial forebrain bundle terminate in the hypothalamic nuclei. Knowledge of the central connections becomes significant in functional MR imaging. Conventional imaging such as X-rays has almost become obsolete in the evaluation of the anterior skull base and olfactory nerve and are increasingly being replaced by CT and MRI. High-resolution helical CT scanner using appropriate technical settings such as small pitches, ultra-thin slices, isotropic voxels, high matrix settings, and high-quality bone reconstruction algorithms allows accurate multi-planar depiction of the anterior skull base and bony olfactory grooves, which demonstrate high variability in shape, size and degree of symmetry. Main indication for CT is trauma because of impeccable depiction of bone but with the inherent limitation of poor soft tissue contrast. CT is indicated in acute indications of maxillofacial/cranial trauma and in chronic indications such as cribriform plate trauma with CSF leakage. Both focal bone disruption and elective filling of the ethmoid cells located beneath the fracture can be depicted in these conditions, with or without the use of iodinated contrast material. CT is also best suited in patients with claustrophobia and other conditions where MRI is contraindicated (e.g.,: in patients with pacemaker device).Modern scanners with inherent dose modulation protocols help in achieving low radiation. In tumours causing bone destruction or remodelling, CT scores over other modalities in accurate depiction of the extent and staging. Volume thin T2-weighted images in Fast Spin Echo (FSE) mode in the coronal plane is the best suited technique for anatomical olfactory tract overview, detection of parenchymal lesions and olfactory bulb volumetry. Whole brain coverage remains mandatory for detecting parenchymal contusions which can be done with T2 and hemosiderin-sensitive T2* sequence. FIESTA and CISS sequences, when used concomitantly, help in best depiction of the nerve as well the subarachnoid CSF spaces. These help in evaluating suspected skull base defects with CSF leakage and avoids the use of ionizing radiation. Olfactory bulb volumetry. The coronal T2 FSE 2 mm slice thickness images are browsed from anterior to posterior. The slices from the first image showing the olfactory bulb to the image where there is abrupt termination of the size of the bulb are noted. The surface of the bulb is drawn with an electronic cursor (Fig. 3.26.14) whose area is given in sq. mm. The values are summed from all the slices and multiplied by 2, to give volume in cubic mm. Normal range of the olfactory bulb volume is 40–60 cubic mm (Fig. 3.26.15).
3.26: The anterior skull base and the first cranial nerve – imaging anatomy and pathology
Abbreviations
Imaging anatomy of the anterior skull base and olfactory nerve
Anterior skull base
Boundaries, bones and foraminae
Foraminae in the anterior skull base
Foramen
Location
Structures Passing Through
Foramen cecum (Fig. 3.26.8A)
Junction between the posterior aspect of the frontal bone and anterior aspect of the ethmoid in the midline.
Emissary vein to superior sagittal sinus from nasal epithelium
Anterior ethmoidal foramen (Fig. 3.26.7A)
Slit between the frontal and ethmoid bone
Anterior ethmoid artery, vein and nerve
Posterior ethmoidal foramen (Fig. 3.26.7B)
Seam between the ethmoid and sphenoid bone
Posterior ethmoid artery, vein and nerve.
Cribriform foraminae (Fig. 3.26.8B)
Nasal vault-ethmoid roof
Olfactory nerve rootlets
Embryology
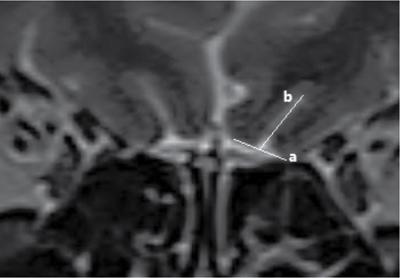
Keros morphology of the olfactory fossa
Cranial nerve one
The olfactory nerve
Introduction.
Neuroanatomy.
Central pathways (Fig. 3.26.14).
Medial forebrain bundle.
Imaging recommendations
Computed tomography (CT).
Magnetic resonance imaging (MRI) of the brain.
Quantitative measurements
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


