Fig. 9.1
Pronator fat plane in a 9-year-old girl. The fat that lies volar to the pronator quadratus muscle is well shown (arrow)
2 Carpal Coalition
Carpal fusion or coalition results from failure of normal segmentation of primitive embryologic mesenchyme. Usually asymptomatic, this occurs in up to 3.6 % of the white American population and is even more common in those of West African descent [2]. It is often familial and bilateral [3]. At times, overlap on radiographs simulates carpal fusion, but evaluation in other projections should clarify this issue. Magnetic resonance imaging (MRI) is rarely necessary. Patients rarely complain of pain or dysfunction unless the fusion is fibrous or crosses carpal rows.
Complete fusion with trabeculae connecting adjacent bones is observed in late childhood or adolescence, but earlier radiographs may demonstrate separate bone nuclei that gradually fuse during maturation. Incomplete fusion has been described in adults, with diminished joint space and small cystic lucencies in the subcortical regions of adjacent bones.
Isolated carpal fusion involves the same row and occurs by far most commonly between the lunate and triquetrum (Fig. 9.2), although occasionally the capitate and hamate fuse [3]. Fusion of other centers, or between carpal bones in different rows, should raise concern for prior infection, an associated systemic disorder (such as Turner’s syndrome, arthrogryposis, or Ellis-van Creveld), or a skeletal dysplasia [4]. In the latter case, brachydactyly, symphalangism, or other anomalies may also be present. Acquired coalition usually indicates prior infection or, more commonly, juvenile idiopathic arthritis (JIA); severe JIA is frequently complicated by multicenter carpal fusion (see Chap. 20).

Fig. 9.2
Lunatotriquetral fusion in a 15-year-old girl. There is solid osseous fusion between the lunate and triquetrum (Courtesy of J. Herman Kan)
3 Amniotic Bands
Congenital amputations may occur when strands of amniotic tissue entrap and constrict fetal parts. The timing determines clinical findings—when early, there is amputation or complete syndactyly, and there may be severe accompanying multisystem involvement. A late event disrupts limb formation to a lesser extent, resulting in fewer amputations and fenestrated syndactyly [5]. Vascular congestion and hemorrhage occur distal to the bands [6], and various malformations result. Incidence is sporadic and varies between 1:1,200 and 1:150,000 births [7, 8]. There is no gender predilection.
Amniotic bands may be completely circumferential or segmental, and they may be shallow or deep enough to cause distal edema or ischemia; occasionally a distal fragment is delivered separately at birth. Defects are usually transverse and unilateral—if bilateral, they are rarely symmetric (Fig. 9.3). If the bands are deep, there may be accompanying vascular abnormalities [7]. MRI delineates soft tissue anomalies as well as vessels and nerves, which can assist surgical planning. Prenatal ultrasound (US) may identify defects and demonstrate bands of amniotic tissue.
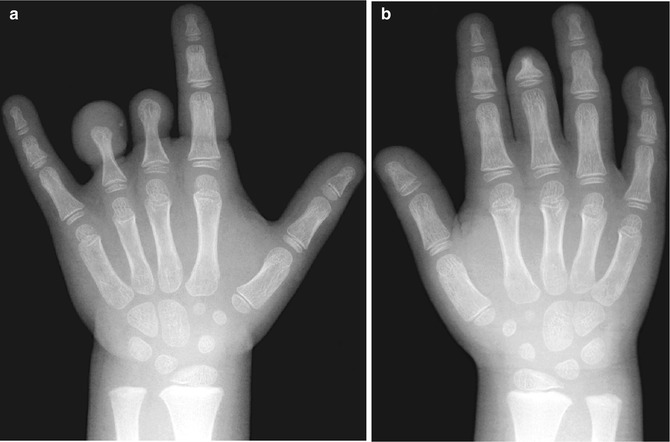
Fig. 9.3
Bilateral congenital amniotic bands. (a) (left) and (b) (right) hands demonstrate bilateral amputations that are more severe on the left (Images copyright Shriners Hospital for Children Northern California)
Constriction defects are most common in the distal extremities, especially the hand. The middle digit is involved most often, and the thumb tends to be spared, perhaps due to fetal positioning (Fig. 9.4) [8]. Severity varies from cutaneous or osseous syndactyly to complete transverse terminal defects (Fig. 9.5). The distal portions of the digits may both amputate and fuse, resulting in acrosyndactyly (Fig. 9.6). Deformed digits may contain complete or incomplete bony units; stubby fleshy rudiments are common. Proximal fusion is often incomplete, resulting in epithelium-lined clefts between the proximal portions of digits [8]. Anencephaly and multiple asymmetric encephaloceles may accompany this abnormality. Clubfoot has been reported in more than one third of cases.


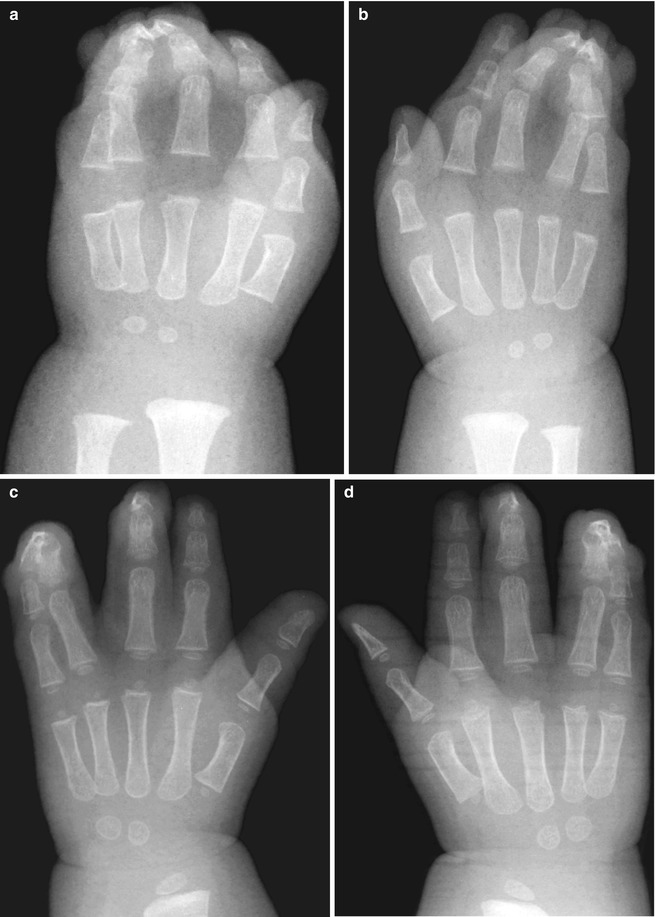
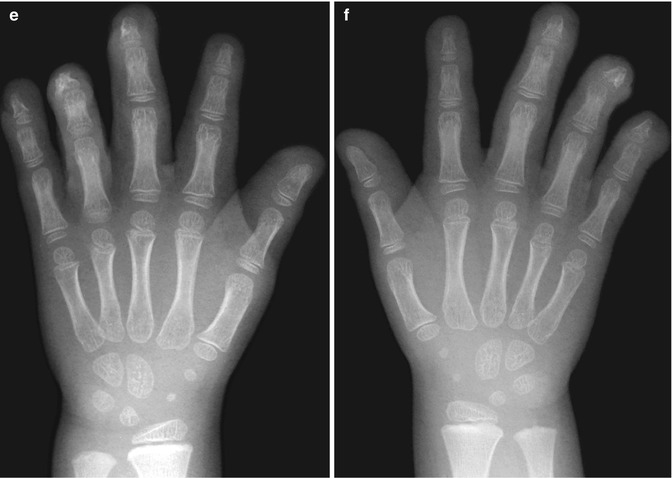
Fig. 9.4
Congenital amniotic bands. The second through fourth rays are amputated at the distal metacarpals, with dysplasia of the fifth finger (Image copyright Shriners Hospital for Children Northern California)
Fig. 9.5
Severe amputation, with minimal first and fifth rays present (Image copyright Shriners Hospital for Children Northern California)
Fig. 9.6
Congenital amputations in a 1-month-old. (a, b) At presentation, there is typical mitten-like syndactyly. (c, d) Two years after surgical separation. (e, f) Three years later, after additional intervention, syndactyly is no longer present (Images copyright Shriners Hospital for Children Northern California)
Differential Diagnosis
Transverse deficiency resembles amniotic band constriction defects. However, transverse deficiency of the hand (symbrachydactyly) is differentiated by the presence of nails and the absence of syndactyly (Figs. 9.7 and 9.8). Similarly, the presence of vestigial digits differentiates transverse deficiency of the forearm from amniotic bands [9] (see Chap. 7).


Fig. 9.7
Symbrachydactyly. There are varying degrees of hypoplasia of the metacarpals, a single phalanx at the thumb, and soft tissue nubbins representing the second through fourth digits. Well-formed nails can be appreciated at the first and third digits and are suggested at the other digits (Image copyright Shriners Hospital for Children Northern California)
Fig. 9.8
Symbrachydactyly in a patient with Poland syndrome. The first through fourth metacarpals are hypoplastic and deformed, and there is symphalangism (arrow) at the fifth ray, as well as syndactyly between the fourth and fifth rays. The first ray is deformed and partially fused (Image copyright Shriners Hospital for Children Northern California)
4 Split Hand
Split-hand defect, also known as cleft hand, may involve all four extremities and is inherited in an autosomal dominant pattern, occasionally skipping generations. Unilateral or sporadic cases are less common (Fig. 9.9). The term ectrodactyly, formerly used synonymously, is not specific for split hand but refers generally to total or partial hand/finger aplasia [4]. Deficiency of radial digits usually accompanies split hand; a strictly median split with all five digits present is rare. Syndactyly or symphalangism is common, and two digits may articulate with one forked metacarpal. A strut-like bone resembling a phalanx may cross from one metacarpal to another (Fig. 9.10). Carpal bones may be fused or absent, and the ulna is occasionally abnormal. The hand tends to function well but is aesthetically quite unusual and so surgery to close the cleft is commonly performed (Fig. 9.10). In addition, any transverse bones should be removed to prevent widening of the cleft, and finger deformities may be treated with rotation osteotomy.


Fig. 9.9
Severe split hand, with markedly diminished ossification. There are only two ossified metacarpals, and both are severely hypoplastic (Image copyright Shriners Hospital for Children Northern California)
Fig. 9.10
Bilateral split hand. (a) The left hand has five metacarpals but only four complete rays. A bony strut expands the base of the proximal phalanx of the third ray, bridging the distal third and fourth metacarpals. (b) The right hand has a similar configuration, except no bone articulates with the hypoplastic third metacarpal. (c) Right hand, after resection of most of the diminutive third metacarpal, the digits are less splayed (Images copyright Shriners Hospital for Children Northern California)
5 Macrodystrophia Lipomatosa (Box 9.1)
Box 9.1: Macrodystrophia Lipomatosa
Hamartomatous overgrowth of mesenchymal elements |
Second and third digits most often |
T1-W: hyperintense fat between linear fibrous hypointense bands |
T2-W: intermediate signal |
Lacks encapsulation, less defined than lipomas |
Macrodystrophia lipomatosa—hamartomatous overgrowth of all mesenchymal elements of the digit including adipose tissue, phalanges, tendons, nerves, and vessels—presents at birth [10]. It is usually unilateral; if bilateral, rarely symmetric. Severe cases may also affect the more proximal portion of the extremity.
Etiology is obscure. Macrodystrophia lipomatosa may result from alteration in somatic cells during limb bud development as well as disturbed fetal circulation [11]. It can be considered to be a localized form of Proteus syndrome, in part because in both conditions PTEN (phosphatase and tensin homolog) is deleted from chromosome 10 [12]. However, although all elements of the finger (blood vessels, tendons, bones, nails) are overgrown, adipose tissue and nerves are especially affected. The adipose tissue is distributed in a mesh of fibrous tissue, involving marrow, periosteum, muscles, nerve sheaths, and subcutaneous tissues. When encountered in the hand, it typically occurs in the distribution of the median nerve, and there may be palmar neuromas or fibrolipomatous hamartomas of the nerve, suggesting it represents a neural disorder, probably related to the sensory nerve distribution pattern. Macrodystrophia lipomatosa does not appear to be inherited and is almost always isolated [13].
Macrodystrophia lipomatosa in the foot is more likely to involve only the phalanges and to demonstrate disproportionate growth; it otherwise behaves and appears similar to the hand [13]. The plantar nerves are often enlarged.
In the hand, multiple osteotomies and debulking procedures can be performed with the goal of cosmesis and good function. However, stiffness almost always eventually develops in the affected digits. If only one digit is involved, ray amputation can be a good option (Fig. 9.11). Additionally, multiple epiphysiodeses can be considered in an attempt to stop longitudinal growth. Amputation is often performed in the foot, with the goal of symmetric shoe size. Premature osteoarthritis may develop in late adolescence.
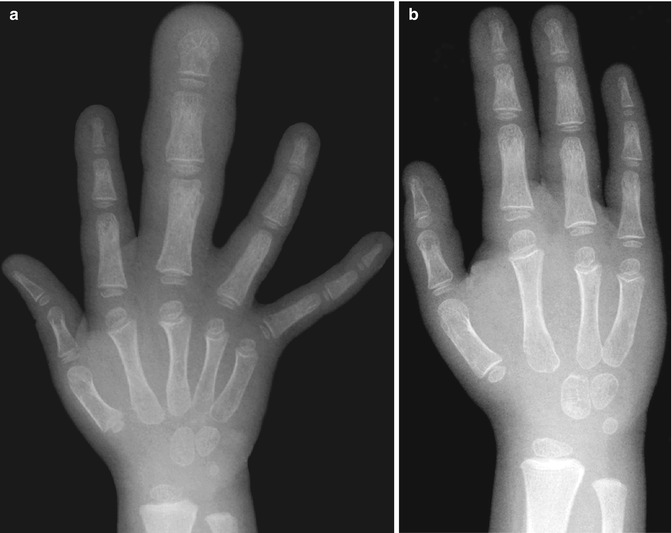
Fig. 9.11
Macrodystrophia lipomatosa in a 3-year-old girl, before and after treatment. (a) The third ray is markedly enlarged, with overgrowth of the bones and soft tissues. Debulking procedures had been unsuccessful. (b) Several months later, it has been resected (Images copyright Shriners Hospital for Children Northern California)
Imaging
The involved digit is enlarged at birth and may develop proportionately or disproportionately. If more than two fingers are involved, syndactyly may be present as well. The second and third digits are affected most often, whereas the fifth is rarely involved (Figs. 9.12 and 9.13). A rare type has associated hyperostosis and apparent osteochondromatous masses [14]. The metacarpals are frequently normal, but may grow disproportionately. The distal ends of the phalanges are splayed, and the phalanges are broad and elongated. Soft tissues are obviously enlarged, with fatty proliferation most pronounced at the palmar/plantar and lateral regions. This contributes to apparent hyperextension and ulnar deviation [13]. Fatty infiltration is visible radiographically and can be confirmed with MRI (Fig. 9.14).


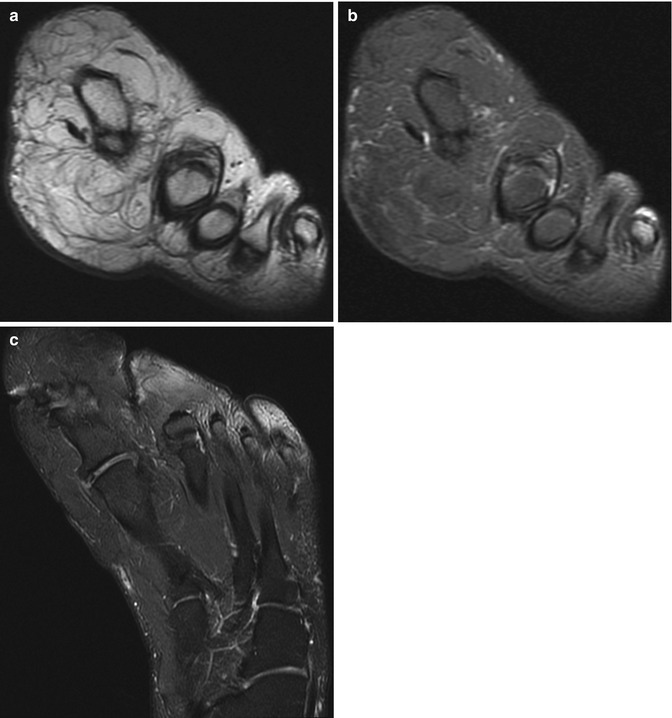
Fig. 9.12
Macrodystrophia lipomatosa in a 6-year-old boy. The phalanges of the third digit (and to a lesser extent the second) are broad and elongated. There is fatty infiltration, with ulnar deviation of the overgrown third ray (Image copyright Shriners Hospital for Children Northern California)
Fig. 9.13
Macrodystrophia lipomatosa involving the second and third rays, with relatively mild bone and soft tissue overgrowth (Image copyright Shriners Hospital for Children Northern California)
Fig. 9.14
Macrodystrophia lipomatosa in a 17-year-old boy. (a) Coronal proton density (PD) MRI through the distal metatarsals demonstrates fatty infiltration of the interosseous spaces; this is hypointense on the corresponding coronal PD fat-suppressed (FS) image (b). An axial PD FS image (c) through the foot demonstrates both osseous and soft tissue hypertrophy
At magnetic resonance imaging (MRI), T1-weighted (T1-W) images show hyperintense fat signal interspersed between linear fibrous hypointense bands; at T2-weighted (T2-W) imaging, most of the tissue demonstrates intermediate signal intensity, following that of fat [15]. The fatty tissue, lacking encapsulation, is less defined than typical lipomas [16]. There may be accompanying fibrolipomatous hamartomas of the nerve, resulting in fusiform enlargement due to fat interspersed between nerve bundles [17]. If there is severe fatty infiltration of the nerve, it may be difficult to differentiate from the surrounding adipose tissue.
Differential Diagnosis
Congenital enlargement of one or several digits may be a local manifestation of a more extensive disease, such as hemangiomatosis, lymphangiomatosis, arteriovenous malformation, Klippel-Trenaunay syndrome, neurofibromatosis, or congenital lymphedema.
6 Symphalangism
Symphalangism refers to the fusion of one phalanx to another within the same digit and presumably results from failure of the joint segment to differentiate (Fig. 9.15). Since this area is cartilaginous in infancy, the lack of segmentation may not be evident radiographically until later, although the interphalangeal space or the physis of the middle phalanx may be narrowed [4]. Clinically, the normal flexion and extension creases in the skin overlying the affected joint are absent from birth. The middle phalangeal physis may fuse prematurely, or the epiphysis may first fuse with the phalanx just proximal to it. Symphalangism is distinguished from syndactyly, which refers to cutaneous or osseous fusion between adjacent digits.
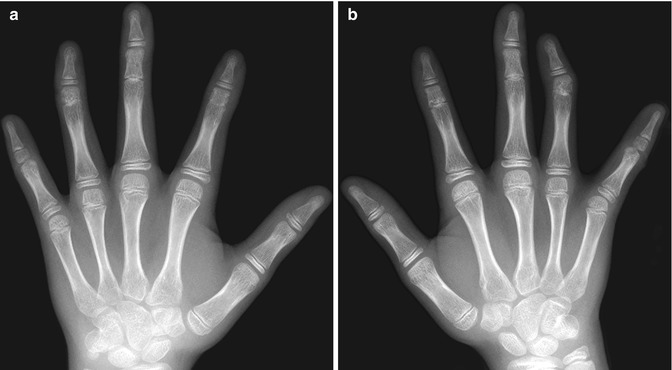
Fig. 9.15
Symphalangism in a 12-year-old girl. (a) (left) and (b) (right) radiographs show the proximal interphalangeal joints of the second through fourth digits are fused to a variable but symmetric extent, with partial clefts evident in the third and fourth digits. The middle phalanges are hypoplastic, and the heads of the metacarpals are flattened (Courtesy of Tal Laor, Cincinnati Children’s Hospital)
Frequently inherited as an autosomal dominant trait, symphalangism can affect both hands and both feet in a bilaterally symmetric pattern. In the hands it characteristically affects the proximal interphalangeal joint (Fig. 9.15), whereas in the feet the distal interphalangeal joint is usually involved. The fifth finger is affected most often, and the thumb is rarely abnormal. The proximal and middle phalanges may be linked by a smooth continuum of bone, but there is frequently expansion at the expected level of the joint, and a partial cleft or irregular lucency may be present. The distal phalanges are often hypoplastic, and the metacarpal heads slightly flattened. The skin around the joint is smooth due to lack of flexion.
Carpal and tarsal fusions accompany symphalangism in many families. In the hand, triquetral-hamate and capitate-hamate fusions are most common; in the foot, talonavicular or calcaneocuboid fusions occur. Syndactyly is often associated, and syndromic cases often have associated acrocephalosyndactyly. Elbow dysplasia may coexist.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


