Key Points
- ▪
The lateral chest radiograph is particularly useful for the recognition of specific chamber enlargement (other than that of the right atrium) for the recognition of the valve prostheses and rings as they are projected away from the spine. Protheses and rings themselves, as well as their location and orientation, are more apparent than on the frontal radiograph, as are pleural effusions, and left lower lobe disease.
- ▪
The normal anterior and posterior border silhouettes of the heart should be familiar.
Cardiovascular Silhouettes on the Lateral Chest Radiograph
As with the frontal chest radiograph, it is important to be familiar with the silhouettes of the cardiopericardial silhouettes (CPS) and major vascular structures on the lateral chest radiograph. Although often ignored, the lateral chest radiograph is particularly useful for valve localization and for the left and right ventricular chamber size assessment ( Graphic 3-1 ).

Normal Anterior Border Silhouettes
In some patients, the anterior border of the right brachiocephalic vein and superior vena cava are visible (from superior to inferior) as the first silhouette on the lateral radiograph.
- □
Ascending aorta: The anterior border of the ascending aorta is usually the first anterior silhouette on the lateral chest radiograph. However, it usually presents as a vague image because of mediastinal fat obscuring the silhouette. The arch of the aorta is usually well defined except where there are adjacent blood vessels (branch vessels and the great veins).
- □
Main pulmonary artery: A small segment of the anterior border of the main pulmonary artery above the pulmonic valve is visible as a less vertically oriented silhouette. It is not normally against the sternum. As with the ascending aorta, it is usually a vague image because of mediastinal fat obscuring the silhouette.
- □
The right ventricular outflow tract: The anterior border of the right ventricular outflow tract is seen as an inferior continuation of the pulmonary artery. The tract and the pulmonary artery cannot be radiographically distinguished.
- □
The right ventricle: The anterior portion of the right ventricle is the lowermost portion of the anterior border of the CPS. Normally, most of it is in contact with the sternum. It is for this reason that sternal and parasternal injury commonly results in right ventricular injury.
Normal Posterior Border Silhouettes
From superior to inferior, the normal silhouettes are as follows:
- □
Aortic arch: The posterior border of the arch of the aorta (outside curvature), and often the arch itself, is visible arcing posteriorly and inferiorly. The inside border is seldom visible.
- □
Left pulmonary artery: The distal portion of the main pulmonary artery and the left pulmonary artery are visible under the aorta.
- □
Left atrium: The posterosuperior and posterior borders of the left atrium form the majority of the posterior border of the CPS.
- □
Left ventricle : The normal basal posterior left ventricle may be seen as an oblique silhouette under the left atrium but does not normally project far behind the inferior vena cava. Note that the posterior border of the inferior vena cava and right atrium may be uncovered with a deep inspiration.
“Narrow anteroposterior diameter” fulfills both of the following criteria:
- □
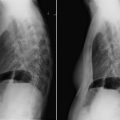
Lateral chest radiograph: Measure from the posterior surface of the sternum to the anteriormost border of a thoracic vertebra. The normal dimension is greater than 8.0 cm ( Fig. 3-1 ).

Figure 3-1
Sagittal contrast-enhanced computed tomography (CT) scans revealing anterior and posterior cardiac silhouettes on the lateral chest radiograph. In the left upper image, the anterior border is formed of the right ventricular anterior wall, the right ventricular outflow tract more superiorly, then the pulmonary valve, and the beginning of the pulmonary artery. The relatively superior position of the left atrium is also seen. In the right upper image (sagittal view to the right side), the inferior vena cava (IVC; non–contrast-enhanced because of dye injection only via the left arm veins) is seen in longitudinal depiction, rising vertically above the diaphragm. The supradiaphragmatic IVC forms an important relation to the posterior wall of the left ventricle, as the position of the IVC varies little due to its tethering by the diaphragm. As well, the left atrium above it is also seen. The left lower image is a sagittal view toward the left of midline revealing the two ventricles in cross-section. The posterior border of the left ventricle is usually nearly as well seen by chest radiography as it is by CT scanning. The right lower image is a superimposition of images with the IVC and the left ventricle depicting how little the (normal) left ventricular posterior wall extends behind the line of the supradiaphragmatic IVC.
- □
Frontal chest radiograph: The ratio of the transverse diameter on frontal CXR to the anteroposterior diameter (as mentioned previously) is greater than 2.7.
Signs of Cardiac Chamber Enlargement on the Lateral Chest Radiograph
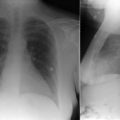
Enlargement of the Left Atrium
The normal left atrial posterior border is formed by pulmonary veins entering into segments of atrial wall and does not have a smooth and regular contour. For this reason, the normal left atrium is vaguely defined on the lateral chest radiograph ( Fig. 3-2 ). An enlarged left atrium forms a more evenly rounded and smooth border and is more clearly seen on the radiograph ( Graphic 3-2 ).