The Normal Mediastinum
W. Richard Webb
The mediastinum is defined as the tissue compartment located between the two lungs, posterior to the sternum, anterior to the vertebral column, and extending from the thoracic inlet to the diaphragm.
CT ANATOMY
The aorta and its branches, the great veins, the pulmonary arteries, and the trachea and main bronchi serve as reliable guides to localizing other important mediastinal structures. As an aid to understanding regional anatomy, the mediastinum can be divided into four compartments, respectively, from superior to inferior: (a) the supraaortic or superior mediastinum; (b) the region of the aortic arch and aortopulmonary window (APW); (c) the pulmonary arteries, subcarinal space, and azygoesophageal recess; and (d) the heart and paracardiac mediastinum.
Supraaortic (Superior) Mediastinum
Just below the thoracic inlet (Fig. 7-1A,B), the mediastinum is relatively narrow from anterior to posterior. The trachea is centrally located.
The esophagus lies posterior to the trachea but can be displaced to the left (more common) or right. It is often collapsed and appears as a flattened structure of soft-tissue attenuation. Small amounts of air or fluid may be seen in its lumen.
Other than the trachea and esophagus, the great arterial branches of the aorta and the brachiocephalic veins are the most apparent normal structures at this level. The brachiocephalic veins are the most anterior and lateral vessels visible, lying immediately behind the clavicular heads. Although they vary in size, their positions are relatively constant.
The right brachiocephalic vein has a nearly vertical course throughout its length. The left brachiocephalic vein is longer and courses horizontally as it crosses the mediastinum (see Fig. 7-1B). The precise cephalocaudal location of this vein is quite variable; although it is most frequently visible at this level, the horizontal portion of the left brachiocephalic vein also can be seen at the level of the aortic arch.
The innominate, subclavian, and carotid arteries lie posterior to the veins and adjacent to the anterior and lateral walls of the trachea. These can be reliably identified by their consistent positions. The innominate (brachiocephalic) artery is located in close proximity to the anterior tracheal wall, near its midline or slightly to the right of midline in most normals; it is the most variable of all the great arteries. The left common carotid artery lies to the left and slightly posterior to the innominate artery; generally it has the smallest diameter of the three major arterial branches. The left subclavian artery is a relatively posterior structure throughout most of its course, lying to the left of the trachea or slightly posterior to its midline. The lateral border of the left subclavian artery typically indents the mediastinal surface of the left upper lobe. Small vascular branches, particularly the internal mammary veins and vertebral arteries, are often seen in this part of the mediastinum.
In some patients, the thyroid gland extends into the superior mediastinum, and the right and left thyroid lobes may be visible on each side of the trachea. On CT, the thyroid can be distinguished from other tissues or masses because of its iodine content; its attenuation is greater than that of soft tissue.
Aortic Arch and Aortopulmonary Window
While the supraaortic region largely contains arterial and venous branches of the aorta and vena cava, this compartment contains the undivided mediastinal great vessels, the aorta and superior vena cava, and also several important mediastinal spaces and lymph node groups (Figs. 7-2,7-3 and 7-4).
The aortic arch has a characteristic but variable appearance (see Fig. 7-2A). The anterior aspect of the arch is located anterior and to the right of the trachea, with the arch passing to the left and posteriorly. The posterior arch usually lies anterior and lateral to the spine. The aortic arch tapers slightly along its length, from anterior to posterior.
The position of the anterior and posterior aspects of the arch can vary in the presence of atherosclerosis and aortic tortuosity; typically the anterior arch is located more anteriorly and to the right in patients with a tortuous aorta, while the posterior aorta lies more laterally and posteriorly, in a position to the left of the spine.
At this level, the superior vena cava is visible anterior and to the right of the trachea, usually being elliptical in shape (see Fig. 7-2A).
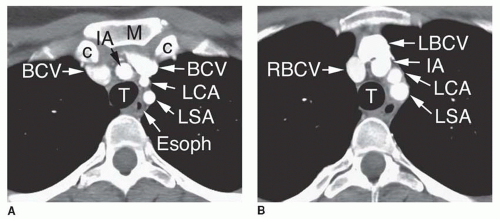 FIG. 7.1. Normal CT anatomy. Supraaortic mediastinum. A: M, manubrium; c, clavicular head; T, trachea; Esoph, esophagus; BCV, brachiocephalic vein; IA, innominate artery; LCA, left carotid artery; LSA, left subclavian artery. B: T, trachea; RBCV, right brachiocephalic vein; LBCV, left brachiocephalic vein; IA, innominate artery; LCA, left carotid artery; LSA, left subclavian artery. |
The esophagus appears the same as at higher levels, being posterior to the trachea but variable in position. Often it lies somewhat to the left of the tracheal midline (see Fig. 7-2A).
The aortic arch on the left, the superior vena cava and mediastinal pleura on the right, and the trachea posteriorly serve to define a somewhat triangular space called the pretracheal space (see Fig. 7-2A and B). This fat-filled space contains mediastinal lymph nodes in the pretracheal or anterior paratracheal chain. Other mediastinal node groups are closely related to this group both spatially and in regard to lymphatic drainage. It is common to see a few normal-sized lymph nodes in the pretracheal space.
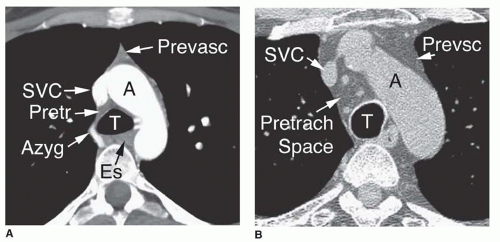 FIG. 7.2. Normal CT anatomy. Aortic arch level. A: Contrast-enhanced CT at a lower level in the same patient as in Figure 7-1. T, trachea; Es, esophagus; A, aortic arch; SVC, superior vena cava; Azyg, azygos arch; Prevasc, prevascular space containing thymus; Pretr, pretracheal space. B: Unenhanced high-resolution CT. T, trachea; A, aortic arch; SVC, superior vena cava; Prevasc, prevascular space; Pretrach, pretracheal space containing normal lymph nodes; Prevsc, prevascular space containing thymus replaced by fat. |
Anterior to the great vessels (aorta and superior vena cava) at this level is another triangular space called the prevascular space (see Figs. 7-2 and 7-3). The apex of this triangular space represents the “anterior junction line” (see Figs. 7-2A, and 7-3A and B). This compartment, which is anterior mediastinal, primarily contains thymus (described in detail below), lymph nodes, and fat (see Figs. 7-2 and 7-3). The mediastinal pleural reflections bordering the prevascular space may be concave or convex laterally, although a marked convexity suggests anterior mediastinal mass or thymic enlargement.
At a level slightly below the aortic arch, the ascending aorta and descending aorta are visible as separate structures
(Fig. 7-3A and C). The average diameter of the proximal ascending aorta averages 3.6 cm (range, 2.4 to 4.7 cm), the ascending aorta just below the arch 3.5 cm (range, 2.2 to 4.6 cm), the proximal descending aorta 2.6 cm (range, 1.6 to 3.7 cm), the mid-descending aorta 2.5 cm (range, 1.6 to 3.7 cm), and the distal descending aorta 2.4 cm (range, 1.4 to 3.3 cm).
(Fig. 7-3A and C). The average diameter of the proximal ascending aorta averages 3.6 cm (range, 2.4 to 4.7 cm), the ascending aorta just below the arch 3.5 cm (range, 2.2 to 4.6 cm), the proximal descending aorta 2.6 cm (range, 1.6 to 3.7 cm), the mid-descending aorta 2.5 cm (range, 1.6 to 3.7 cm), and the distal descending aorta 2.4 cm (range, 1.4 to 3.3 cm).
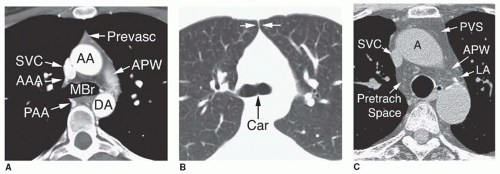 FIG. 7.3. Normal CT anatomy. Aortopulmonary window level. A: Contrast-enhanced CT at a lower level in the same patient as in Figures 7-1 and 7-2A. MBr, main bronchi at the level of the carina; AA, ascending aorta; DA, descending aorta; SVC, superior vena cava; AAA, anterior azygos arch; PAA, posterior azygos arch; Prevasc, prevascular space containing thymus; APW, aortopulmonary window with volume averaging of superior aspect of the left pulmonary artery. B: Lung window scan, same level as (A). The tracheal carina (carina) is visible. The apex of the triangular prevascular space represents the anterior junction line (white arrows). The mediastinal pleural reflections bordering the prevascular space are concave laterally. C: Unenhanced high-resolution CT at a lower level in the same patient as in Figure 7-2B. A, ascending aorta; SVC, superior vena cava; PVS, prevascular space containing thymus replaced by fat; Pretrach Space, pretracheal space containing normal lymph nodes; APW, aortopulmonary window containing normal lymph nodes; LA, ligamentum arteriosum. |
At or near this level, the trachea bifurcates into the right and left main bronchi. Near the carina, the trachea commonly assumes a somewhat triangular shape (see Fig. 7-2A). The carina is usually visible on CT (see Fig. 7-3A and B).
On the right side, the azygos arch arises from the posterior wall of the superior vena cava, passes over the right main bronchus, and continues posteriorly along the mediastinum to lie to the right and anterior to the spine (see Figs. 7-2A and 7-3A). Below the level of the azygos arch, the azygos vein is consistently seen in this position. The azygos arch is often visible on one or two adjacent slices and sometimes appears nodular. However, its characteristic location is usually sufficient to allow its correct identification. When the azygos arch is visible, it marginates the right border of the pretracheal space.
The APW is located on the left side of the mediastinum, caudal to the aortic arch but cephalic to the main pulmonary artery (see Fig. 7-3A and C). The APW contains fat, lymph nodes, the recurrent laryngeal nerve, and the ligamentum arteriosum; the latter two are usually invisible. In some patients, the APW is not well seen, with the main pulmonary artery lying immediately below the aortic arch.
The superior pericardial recess, containing a small amount of pericardial fluid, is often visible in the pretracheal space immediately behind the ascending aorta (see Fig. 7-4A). Although it is sometimes confused with a lymph node, its typical location, contact with the aortic wall, oval or crescentic shape, and relatively low (water) attenuation allow it to be distinguished from an abnormality. The anterior recess of the pericardial space is sometimes seen anterior to the aortic arch, ascending aorta, and pulmonary artery (see Fig. 7-4B).
Pulmonary Arteries, Subcarinal Space, and Azygoesophageal Recess
At or near the level of the tracheal carina or main bronchi, the main pulmonary artery divides into its right and left branches (Fig. 7-5A to C). The left pulmonary artery is somewhat higher than the right, usually being seen 1 cm above it, and appears as the continuation of the main pulmonary artery, directed posterolaterally and to the left (see Fig. 7-5A and B). The right pulmonary artery arises at nearly a right angle to the main and left pulmonary and crosses the mediastinum from left to right, anterior to the carina or main
bronchi (see Fig. 7-5B and C). The right pulmonary artery limits the most caudal extent of the pretracheal space and the anterior aspect of the subcarinal space.
bronchi (see Fig. 7-5B and C). The right pulmonary artery limits the most caudal extent of the pretracheal space and the anterior aspect of the subcarinal space.
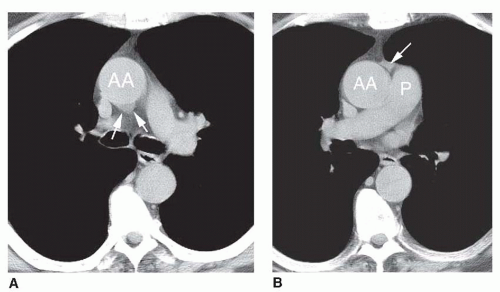 FIG. 7.4. Normal superior pericardial recess. Unenhanced CT. A: The superior pericardial recess (arrows) is visible posterior to the ascending aorta (AA) in the precarinal space. B: At a lower level, the anterior reflection of the superior pericardial recess (arrow) is visible in the groove between the ascending aorta (AA) and main pulmonary artery (P). |
The azygos vein parallels the esophagus along the right side of the mediastinum and laterally contacts the medial pleural reflections of the right lower lobe, defining the posterior border of the azygoesophageal recess (see Fig. 7-5A to C). On the left side, the hemiazygos vein parallels the descending aorta, lying posterior to it (see Fig. 7-5A to C); it is not always visible. The hemiazygos vein generally drains into the azygos vein via a branch that crosses the midline behind the aorta, near the level of the T8 vertebral body. This branch is sometimes seen on CT in normal individuals.
The subcarinal space is the region of the mediastinum immediately below the carina, marginated laterally by the main bronchi. It contains a number of lymph nodes and is closely related to the esophagus (see Fig. 7-5B and D).
Below the level of the tracheal carina and azygos arch, the medial aspect of the right lung contacts the mediastinum in close apposition to the azygos vein, esophagus, and subcarinal space. This region of the mediastinum is called the azygoesophageal recess (see Fig. 7-5C and D). The contour of the azygoesophageal recess is concave laterally in the large majority of normal subjects; a convexity in this region should be regarded as suspicious of mass and the scan examined closely for a pathologic process. However, a convexity in this region may also be produced by a prominent normal esophagus or azygos vein and is particularly common in patients with a narrow mediastinum and in children.
Normal nodes are commonly visible in the subcarinal space, being larger than normal nodes in other parts of the mediastinum and up to 1.5 cm in short-axis diameter (see Fig. 7-5D). The esophagus usually is seen immediately posterior to the subcarinal space, and distinguishing nodes and esophagus may be difficult unless the esophagus contains air or contrast material, or its course is traced on adjacent scans.
Heart and Paracardiac Mediastinum
At the level of the heart, the prevascular mediastinum becomes thin or is obliterated by the heart contacting the anterior chest wall (Fig. 7-6). Little soft tissue is visible anterior and lateral to the cardiac chambers and origins of the main pulmonary artery and aorta. However, posterior to the heart, the azygoesophageal recess remains visible to the level of the diaphragm. As at higher levels, the contour of the azygoesophageal recess is concave laterally, closely opposed to the esophagus and azygos vein. Posterior to the descending aorta, fat, the hemiazygos vein and small lymph nodes occupy the left paravertebral space. The right paravertebral space is considerably thinner or invisible.
PLAIN RADIOGRAPHIC ANATOMY
On frontal (posteroanterior [PA] or anteroposterior [AP]) chest films, five important mediastinal structures should be easily identified (Fig. 7-7). In addition to their intrinsic importance in diagnosis, these structures serve to anchor a number of important mediastinal stripes, lines, and interfaces and orient the observer to specific mediastinal regions and compartments that are important in diagnosis. These structures are as follows:
Trachea, tracheal carina, and main bronchi
Aortic arch
Main pulmonary artery
Azygos vein
Heart and its chambers
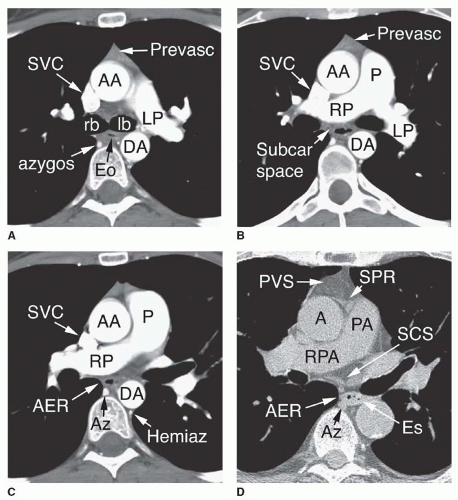 FIG. 7.5. Normal CT anatomy. Level of the pulmonary arteries, subcarinal space, and azygoesophageal recess. A: Contrast-enhanced CT at a lower level in the same patient as in Figures 7-1, 7-2A, and 7-3A. rb, right main bronchus; lb, left main bronchus; AA, ascending aorta; DA, descending aorta; SVC, superior vena cava; azygos, azygos vein; Eo, esophagus; Prevasc, prevascular space containing thymus; LP, left pulmonary artery. B: Contrast-enhanced CT slightly below level shown in (A). AA, ascending aorta; P, main pulmonary artery; LP, left pulmonary artery; RP, right pulmonary artery; DA, descending aorta; SVC, superior vena cava; Prevasc, prevascular space containing thymus; Subcar space, subcarinal space. C: Contrast-enhanced CT slightly below level shown in (B). AA, ascending aorta; P, main pulmonary artery; RP, right pulmonary artery; DA, descending aorta; SVC, superior vena cava; Az, azygos vein; Hemiaz, hemiazygos vein; AER, azygoesophageal recess. D: Unenhanced high-resolution CT at a lower level in the same patient as (B) and (C). A, ascending aorta; PA, main pulmonary artery; RPA, right pulmonary artery; PVS, prevascular space containing thymus replaced by fat; SPR, anterior superior pericardial recess; SCS, subcarinal space containing normal lymph nodes; AER, azygoesophageal recess; Az, azygos, vein; Es, esophagus. |
Trachea, Tracheal Carina, and Main Bronchi
The trachea extends from the inferior aspect of the cricoid cartilage to the tracheal carina. It is 10 to 12 cm in length in most individuals. It is divided into extrathoracic and intrathoracic portions at the point it passes posterior to the manubrium (see Fig. 7-7).
The trachea may appear to have a slightly serrated wall because of indentations on the tracheal air column adjacent to the tracheal rings. On the lateral view, serration is seen only along the anterior tracheal wall, as the posterior wall lacks cartilage. Calcification of tracheal cartilages is common in older patients, particularly women. Slight tracheal narrowing with an indentation on the left aortic wall is often seen at the level of the aortic arch.
The tracheal carina is visible at the bifurcation of the trachea into right and left main bronchi. The carina is usually seen
near the level of the undersurface of the aortic arch. The right and left main bronchi are usually both visible, with the right main bronchus appearing more vertical than the left. The angle between the inferior walls of the main bronchi, the carinal angle, is variable, ranging from about 35 to 90 degrees.
near the level of the undersurface of the aortic arch. The right and left main bronchi are usually both visible, with the right main bronchus appearing more vertical than the left. The angle between the inferior walls of the main bronchi, the carinal angle, is variable, ranging from about 35 to 90 degrees.
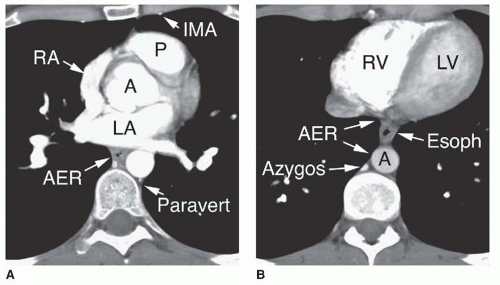 FIG. 7.6. Normal CT anatomy. Level of the heart and paracardiac mediastinum. A: Contrast-enhanced CT at a lower level in the same patient as in Figures 7-1, 7-2A, 7-3A, and 7-5A,B,C. A, aortic root; P, pulmonary outflow tract; RA, right atrium; LA, left atrium; AER, azygoesophageal recess; Paravert, left paravertebral space containing hemiazygos vein; IMA, internal mammary artery. B: Contrast-enhanced CT below the level of (A). RV, right ventricle; LV, left ventricle; AER, azygoesophageal recess; A, descending aorta; Azygos, azygos vein; Esoph, esophagus. |
Aortic Arch
The appearance of the aorta is characteristic, although it can vary in size and shape. The thoracic aorta is usually considered to consist of an ascending segment, a transverse segment or arch, and a descending segment.
The aortic arch begins at the innominate artery and consists of two parts. The proximal part of the arch is the longer and gives rise to the innominate, left carotid, and left subclavian arteries, although variations in the branching pattern of these vessels and their divisions are common. The distal part of the arch, between the origin of the left subclavian artery and the ligamentum arteriosum, is known as the aortic isthmus; it is relatively short, measuring 1 to 2 cm in length, and its lumen may be a few millimeters narrower in adults than the aorta immediately distal to the ligamentum. The descending thoracic aorta is distal to the ligamentum arteriosum.
On frontal radiographs, the lateral aspect of the aortic arch (the “aortic knob”) is typically visible through about half of its circumference (see Fig. 7-7). The lateral edge of the aortic arch visible on radiographs usually represents the edge of the posterior arch. Although it is tempting to measure the aortic diameter as the distance between the edge of the tracheal air column medially and the interface between aorta and lung laterally, these lie in different planes and this measurement is not necessarily valid.
Main Pulmonary Artery
The main pulmonary artery arises at the base of the right ventricle and extends superiorly for a distance of approximately 5 cm before dividing into the right and left pulmonary arteries. The main, right, and left pulmonary arteries are intrapericardial. The main pulmonary artery divides into right and left pulmonary arteries posterior to the ascending aorta and anterior to the main bronchi.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


