Two adjacent foramina form one large common foramen. Hypoplasia of the anterior transverse process associated. On frontal radiographs, the pedicle is missing.
In the cervical column, neurologic or vascular symptoms in upper extremity common (“absent cervical pedicle syndrome”), MRI will demonstrate the courses of the involved nerve roots. Thoracic and lumbar are most often asymptomatic variations.
Smooth-bordered widening on the lateral image; wide foramen on the oblique images. MRI for full examination.
Commonly neurofibromas or neuroblastoma, ganglioneuroma, or schwannoma. Others: teratoma, lipoma, LCH, hemangioma, vascular malformation, spinal epidural cyst.
Serpiginous vertebral artery
Simulates the dumbbell tumor configuration.
Delineation of vessel by MRA.
NF1 lateral meningocele
Widened dural sac. Soft-tissue density mass along the spine.
Café-au-lait spots on skin.
Nerve root diverticulum
Traumatic in origin.
CT or MRI.
Hypertrophic interstitial polyneuritis
Thickening of the nerves causes erosion of the neural arches with flattening of the upper edges. May have concave posterior vertebral bodies; wide interpedicle distance.
Déjerine-Sottas syndrome. Onset usually in childhood. MRI for definition.
Fig. 4.244a, b Absent cervical pedicle at right C4. (a) Right posterior oblique view: there are common intervertebral foramina from C3–C5 (arrowheads). Through it is seen a hypoplastic C4 transverse process. Arrow shows the right lamina, which is displaced outward and is no longer in line with its fellow laminae. (b) Left posterior oblique, the C4 pedicle is lacking (arrow).Fig. 4.245 “Hourglass/dumbbell” tumor (neurofibroma). Widening of the intervertebral foramen caused by intraspinal and extraspinal “hourglass” or “dumbbell” tumor (neurofibroma). However, unlike the case of absent pedicle (see Fig. 4.240), the consecutive laminae en face maintain a smooth alignment.L Thinning and deformity of the lamina
Table 4.86 Small intervertebral foramen
Diagnosis
Findings
Comments
Congenital anomaly
Fewer nerve rootlets exit through it than a usual foramen.
Often associated with other anomalies: Klippel-Feil syndrome, vertebral fusions, diastematomyelia, and meningomyelocele, for examples.
Posttraumatic
Bony fragments.
CT for bone; MRI for cord and nerve roots.
Osteoarthrosis
Less common in children unless predisposing condition or repeated activity (e.g., cervical area in wrestlers).
Bone laid down into neural canal as part of the degenerative process.
Acquired fusion of vertebral bodies, arches, and apophyseal joints.
Especially in cervical spine area. Formerly juvenile rheumatoid arthritis and juvenile chronic arthritis.
Anomalies at the craniocervical junction
Hox gene effects.
Iatrogenic fusion of the neural arch with bone chips
A possible late complication is pseudarthrosis at the level of the fusion.
Fusion also after surgical stabilization of high-grade scoliosis.
22q11.2 deletion
One finding is occipital assimilation of C1 elements.
Diastematomyelia
Fusion of one lamina to a subjacent lamina.
Unilateral congenital fusion
May lead to progressive scoliosis, especially unilateral vertical pedicle bar.
Close follow-up for progressive curves.
Fig. 4.246a, b Juvenile idiopathic arthritis (JIA). (a) At age 6 years, there are no abnormal fusions. (b) At age 16 years, there is bony fusion of C1 arch and C2, the neural arches of C2 and C3, as well as the dens with the occiput.
Table 4.88 Disruption of the contour of the neural arch (clefts, defects, and fractures)
Diagnosis
Findings
Comments
Normal finding
The neurocentral synchondrosis between the neural arches and the body ossifies between 3 and 6 y of age, but remains patent in approximately 2% of individuals. Midline clefts of the thoracic posterior arches fuse sequentially caudocranially in the first 2 y of life; they can remain visible in some children after age 7 y, and then fuse in adulthood. Isolated defects in the neural arch can occur in the cervical and thoracic vertebrae (and be available for forensic identification if known).
Defects in the posterior neural arch can be associated with cleft palate. Median clefts in the neural arch are common in cleidocranial dysplasia, with delayed closure of the neuro-central synchondrosis.
Narrow midline cleft represents delayed or absent posterior bony union of the laminae. L5 may normally remain ununited until age 10 y, or even later.
No clinical significance unless associated with a dysraphism (skin changes, dermal sinus, progressive foot deformities, for example).
Spina bifida aperta
Associated meningomyelocele or other neural posterior deformities.
MRI for definition. Ultrasound in infancy for associated tethered cord.
Dermal sinus
Fig. 4.248
In lumbosacral midline, rarely occipital. US in infants to confirm or exclude a fistulous connection to the spinal canal. MRI provides the best delineation.
Skin dimple; may be noticed because of a hairy patch or pigmentation. A true fistula may have recurrent meningitis. The fistula can be demonstrated with sterile contrast injection.
Midline cleft common in the posterior arch of C1. Also, lateral clefts (neurocentral synchondroses). The absence of displacement of the anterior lucent fat stripe differentiates C1 anterior clefts from fracture.
Asymptomatic. No specific history of trauma.
Fractures
Uncommon in the neural arches and transverse processes.
Oblique images may show; CT is more specific.
Child abuse a possible cause in infants.
Cervical vertebral fractures
Uncommon in the neural arch prior to age 15 y. Hangman fracture through the pedicles of C2, anterior displacement of the vertebral body. Jefferson fracture of C1: burst fracture with lateral displacement of the lateral masses > 3 mm on axial CT.
Associated widening of the prevertebral soft- tissue space. Caution: a pseudo-Jefferson fracture in many children up to age 4 y: widening of the atlas < 3 mm in the absence of a fracture, the synchondrosis still patent.
Pseudarthrosis after spinal fusion for scoliosis or kyphosis repair
A break in the fusion mass. Consider when abnormal curvature recurs.
Bone scintigraphy more than 6 months after surgery may be confirmatory.
Multiple stippled epiphyses
Coronal cleft in spinous processes.
Also known as chondrodysplasia punctata.
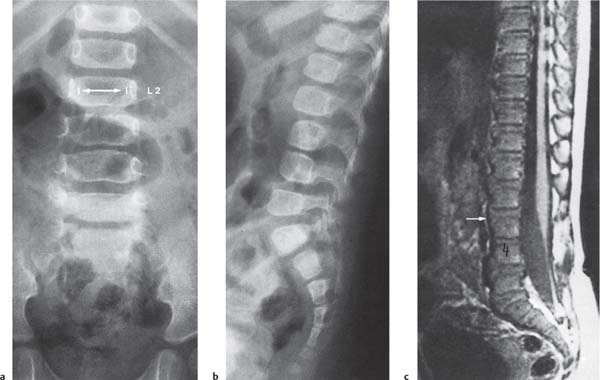
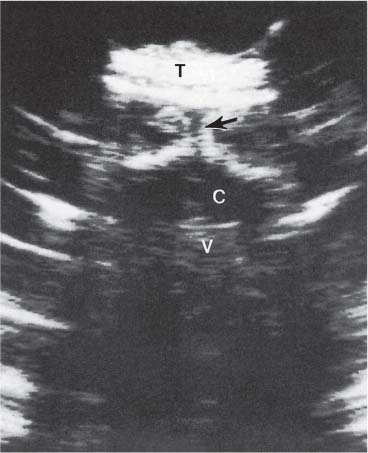
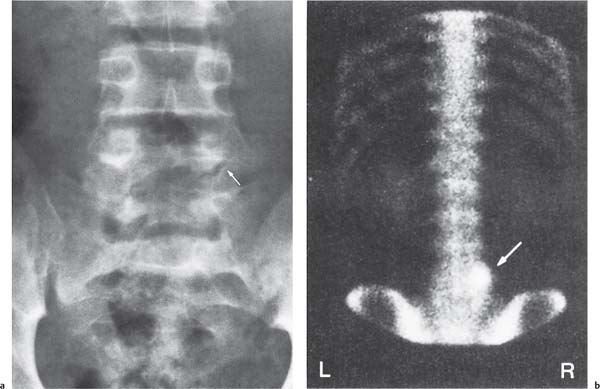
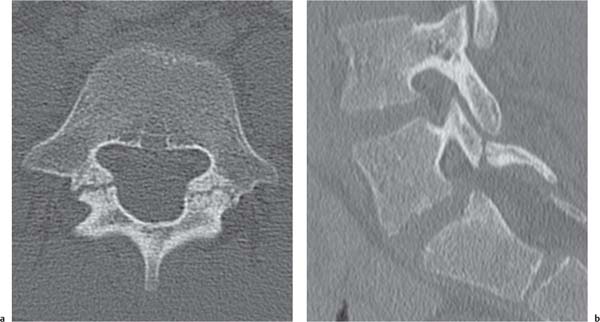
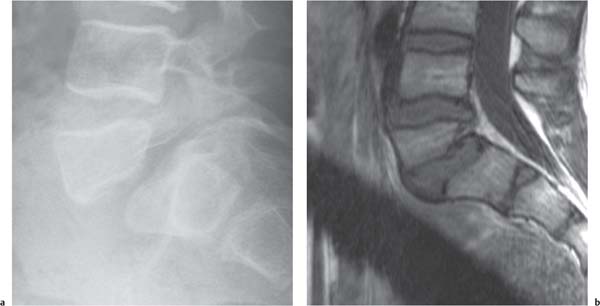
Fig. 4.247a–c Spina bifida with externally visible finding in a 1-year-old boy. Clinically, hypertrichosis over the lower lumbar spine; neurologically intact. (a) Widened lumbar spinal canal, interpedicle distance (double arrow) of 25 mm at L2, 29 mm at L3 and L4, and 30 mm at L5. Some pedicles narrow. Disk space is narrowed at L3–L4. (b) Lateral view, hypoplastic bodies L3 and L4 with narrow disk space between. (c) MRI: the posteriorly tethered spinal cord has conus at L3-L4 (arrow).Fig. 4.248 Neural canal-cutaneus fistula. Historic sonographic examination in a neonate. Arrow points to a fistula.C Spinal canalT Subcutaneous tissueV L3 vertebral bodyFig. 4.249 Neural arch clefts in C2 and C3 (black arrows) in a 2-year-old girl. The anterior fat stripe (white arrow) is not displaced. Apposing bone surfaces are smooth. There is no recent remarkable trauma. Appearance is also unchanged from a prior study, so they are not believed to be fractures.Fig. 4.250a, b Spondylolysis. (a) Interruption of the interarticular pars of L5 (arrow), a hypoplastic left pedicle, and a somewhat dense right pedicle. Clinically, the patient complains of back pain. (b) Classic bone scintigram: increased activity in the right pedicle (arrow) due to stress related to the left spondylolysis.Fig. 4.251a, b Spondylolysis and spondylolisthesis. (a) Axial CT image on this 14-year-old boy shows bilateral irregular lucencies across the pars of the arch of L5, with some sclerosis to either side of the gap. (b) Sagittal reconstruction of the CT shows one-sided L5 spondylolysis and the associated grade 1 spondylolisthesis of L5 on S1.Fig. 4.252a, b Spondylolysis and spondylolisthesis. This is more severe than in Fig. 4.251a, b. (a) The more severe spondylolisthesis of L5 on S1 on the plain image is considered grade 3 of 4 (over 50% relative displacement). (b) T1 MRI reveals the effects on disks and canal contents in this 12-year-old boy with back pain.
Table 4.89 Enlargement of the neural arches
Diagnosis
Findings
Comments
Normal variants
Tendency for development of a large anterior arch of C1 in conjunction with a small posterior arch, and vice versa.
Bone tumors
Expansion of the neural arch together with simultaneous destruction. May narrow the adjacent intervertebral foramen.
Osteoblastoma, aneurysmal bone cyst, giant cell tumor, osteochondroma, hemangioma, and lymphangioma, for example.
Generalized bone disease
Generalized enlargement in involved skeletal elements in, for example, FD or hyperphosphatasemia
Associated changes in the limb bones.
Unilateral enlargement of a pedicle
The contralateral pedicle undergoes hypertrophy in contralateral unilateral spondylolysis or in congenital absence of contralateral pedicle.
Also may occur as an isolated anomaly.
Congenital hyperplasia of anterior tubercle of transverse process
Typically occurs at C5 and C6.
Neurologic symptoms can accompany. Clarification with CT; MRI for evaluation of the cord and nerve roots.
Table 4.90 Abnormal shape of pedicles
Diagnosis
Findings
Comments
Normal variant
Flattening of the usually ovoid shape on front projection, mainly in the upper lumbar spine. The medial boundaries are not quite concave.
If necessary, MRI to exclude an intraspinal process.
Intraspinal mass
Flattening or concavity of the medial border; possible destruction or total obliteration of the neural arch.
MRI for evaluation.
Dysplastic or small pedicle
In various anomalies of vertebral column, especially rachischisis, postirradiation, and in NF1.
Achondroplasia
Short pedicles (and laminae).
Slowing of enchondral growth.
Hypochondroplasia
Less severely short than achondroplasia.
Less severely slowed than achondroplasia.
Melnick-Needles syndrome
May have very small pedicles, especially in the lumbar region. The arches are intact, however.
Osteodysplasty. Thin irregularly marginated ribs.
Postirradiation
Abnormally small pedicles may be part of the acquired growth disturbance.
Associated scoliosis if radiation fields were not symmetrically balanced.
Table 4.91 Destruction, sclerosis, and absent pedicles
CT shows abnormal bone structure. MRI for better definition of soft tissues and any intraspinal canal pathology.
Metastases, leukemia, Hodgkin disease, LCH, osteoblastoma, Ewing sarcoma, osteogenic sarcoma, among others. Among infections, be on the lookout for community-acquired methicillin-resistant Staphylococcus aureus.
Osteoid osteoma
Sclerosis of one pedicle and nearby.
CT, bone scintigraphy. Night pain relieved by aspirin. Secondary scoliosis eventually.
Engelmann disease
Pedicle periosteal reaction leads to dense pedicles.
Progressive diaphyseal dysplasia.
Sclerotic tumors
Sometimes seen in Ewing sarcoma, Hodgkin sarcoma, osteogenic sarcoma, and some metastases.
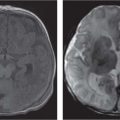
Fig. 4.253a, b Osteoblastoma. (a) Axial CT shows the expansile relatively low-density lesion in the lamina region in this 8-year-old with localized pain. (b) On sagittal T2 MRI to the left of midline, note the high intensity associated with the osteoblastoma.Fig. 4.254 Osteoblastoma obliterating visualization of pedicle. Osteoblastoma replaced the pedicle bony substance (arrow) and caused obstruction of the CSF flow at that level.
Abnormalities in Alignment and Position
Abnormalities in alignment and position include scoliosis, kyphosis, lordosis, and dislocation.
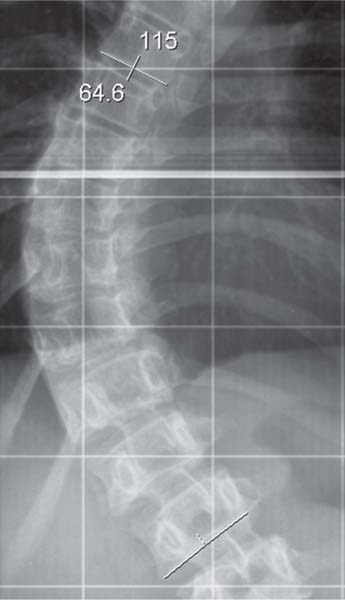
Rotation of vertebrae around the long axis is a key element in lateral curvature. Cobb technique for measuring the angle of the scoliosis (Fig. 4.255). As scoliosis and rotation of bodies progresses, wedging of the body shape occurs.
S-shaped deformity, convex right in the thoracic region is one classic curve. Erect radiographs in two projections are standard. Functional radiographs (lateral bending or perhaps longitudinal stretching) to evaluate the flexibility of curves.
Mostly becoming apparent after the age of 2 y, and especially in second decade. Tendency to progress during growth spurts. Girls much more common than boys. Underlying causes must be excluded, such as NF1, congenital hemivertebra, and intraspinal pathology.
Infantile idiopathic scoliosis
Compensatory, mild (Cobb angle below 15°). Rule out segmentation abnormality such as hemivertebra). Spontaneous regression in first or second year of life.
Believed not uncommonly to be caused by intrauterine position of the fetus; may have concomitant asymmetry of skull, thorax, or pelvis. Other simulator: active infant during imaging.
Fig. 4.255 Cobb method of angle measurements, using end plates most tilted from the horizontal. The severe thoracolumbar curve m easures 65°.
Table 4.93 Scoliosis arising from bony abnormalities
Diagnosis
Findings
Comments
Vertebral malformations (hemivertebrae, etc.)
Fixed scoliosis. A single lateral hemivertebra will result in a locally angulated scoliosis.
May be a part of VATER association.
Asymmetric lumbosacral transitional vertebra
Frontal view: unilateral fusion of a wide transverse process of L5 with S1.
May also occur without scoliosis. Role in any back pain not established.
Anomalies with hemihypertrophy
Asymmetric vertebral development possible. Upright images to show associated pelvic tilt from leg-length discrepancy.
For example, Klippel-Trénaunay syndrome, Weber syndrome, and Proteus syndrome.
Following vertebral fractures
Scoliosis convex to fractured lumbar transverse processes.
Similar possible scoliosis after unilateral rib resection.
Postirradiation
Scoliosis may be due to underdevelopment of the muscles on unilaterally irradiated side (e.g., after treatment of Wilms tumor).
Can occur after doses of 30 Gy, regularly occurs after 40 Gy; latent period up to 10 y.
Spondylolysis, spondylolis-thesis
May coincidentally accompany scoliosis or cause the scoliosis.
Oblique plain images or CT to image.
One hypoplastic lower extremity
Following polio; embryologic reduction deformities in lower extremity sclerotomes. Pelvic tilt on upright images.
Asymmetric thalidomide effect, for example. Any cause of unilaterally shortened lower extremity will lead to functional scoliosis.
Painful scoliosis, not fully flexible in severe cases; the circumscribed increased density may be elusive on plain images.
Bone scintigraphy is most useful way to detect. CT and MRI may also be subtle.
Osteoblastoma
Tumor in body or arch.
Larger than osteoid osteoma.
Lateral block vertebra or vertical pedicle bar
The old conventional tomography showed the fusions well; now may need CT with coronal reconstruction.
Pedicle bar: rapidly progressive scoliosis. Therapy: fusion of the other side.
Spondylocostal dysplasia
Multiple rib and vertebral anomalies.
Also known as Jarcho-Levin syndrome.
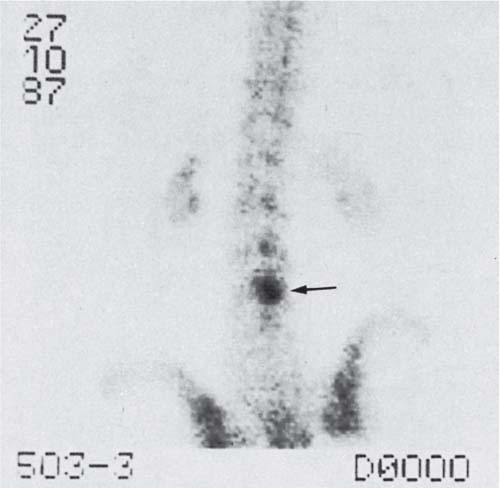
Fig. 4.256 Scoliosis associated with osteoid osteoma in an 11-year-old boy. Bone scintigram: Circumscribed increased uptake in the neural arch of L4 (arrow). Clinically presents as painful fixed scoliosis. CT and MRI had initially been considered unremarkable.
Table 4.94 Spinal and neuromuscular scoliosis causes
Diagnosis
Findings
Comments
Meningomyelocele and related conditions
Often associated with progressive scoliosis.
Other neuromuscular conditions
Often especially long curves (many vertebral levels).
Seated or standing images helpful.
Syringomyelia, hydromyelia
Diagnosed with MRI.
Consider if rapid worsening of scoliosis after surgery or trauma.
Diastematomyelia
A spur is often present (but frequently overlooked) on a frontal radiograph. Scoliosis may result from associated vertebral anomalies. Wide interpedicle distance; vertical fusion of laminae on one side.
Definitive diagnosis with MRI, although CT good for bony spur. Occasionally accompanied by Sprengel deformity of scapula.
Space-occupying lesion in the spinal canal
May show local canal widening on plain images; diagnosis with MRI.
Painful scoliosis with neurologic manifestations. Among tumors, astocytoma is relatively common.
Kyphosis
Kyphosis occurs frequently as a part of kyphoscoliosis in neuro-muscular diseases and in several skeletal dysplasias.
Other kyphosis arises from malformation syndromes with anterior wedging of vertebral bodies, such as Morquio disease.
Kyphosis may be associated with intraspinal abnormalities (Fig. 4.257).
Fig. 4.257 Kyphosis associated with arachnoid cyst. Back pain and worsening kyphosis in a 13-year-old girl. Arachnoid cyst just below the apex of the kyphos shows high intensity on T2 MRI. Did the arachnoid cyst cause the kyphosis, or is it the other way around?
Table 4.95 Kyphosis
Diagnosis
Findings
Comments
Scheuermann “disease,” adolescent kyphosis
Anterior wedging in thoracic vertebrae, classically at least three adjacent levels; irregular end plates.
May lead to early degenerative disk disease (in the fourth decade). Often at least one parent also has Scheuermann kyphosis.
Vertebral body fractures
Anterior wedging as loss of height.
MRI for associated cord damage.
Late sequela of spondylitis (pyogenic or tuberculous)
Wedged kyphosis due to vertebral body destruction and loss of height with possible disk destruction.
Gibbus formation, particularly in tuberculosis, in which case it is known as Pott disease.
For example, because of cervical column neurofibroma surgery.
Achondroplasia
Kyphosis increases with age, independent of the lumbar lordosis.
One more reason for short stature in achondroplasia.
LCH
Kyphosis may precede frank vertebra plana.
Eosinophic granuloma.
Obesity
In overweight children, a tendency to cervical kyphosis.
Chronic lung disease
Develop barrel-shaped thorax.
As examples, asthma and cystic fibrosis.
Severe cervical kyphosis in diastrophic dysplasia, c amptomelic dysplasia, and other dysplasias
Images of chest or cervical spine should include laterals at least once.
Diastrophic dysplasia: hitchhiker thumbs; camptomelic: congenital bent limbs.
Posterior hemivertebra
May be partially compensated for in alignment by anterior overgrowth of adjacent vertebral bodies.
Hox gene effect.
Larsen syndrome
Many vertebral anomalies, which may cause cervical or thoracic kyphosis and other deformities of the region.
Multiple dislocations of joints in the extremities at birth. Overabundant carpal and tarsal bones.
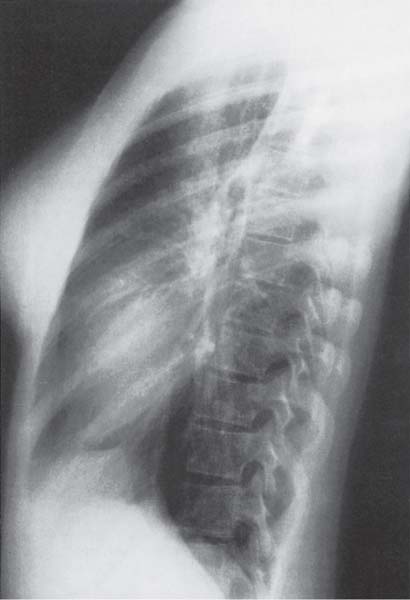
Fig. 4.258 Kyphosis following cervical laminectomy (NF1). Lateral plain image of a 10-year-old who had had a cervical neuroblastoma in the spinal canal.
Table 4.96 Hyperlordosis
Diagnosis
Findings
Comments
Achondroplasia
Increased lordosis at lumbosacral junction.
Sacrum may be seen en face on frontal images.
Idiopathic scoliosis
Curvature changes in all three dimensions in scoliosis.
Associated with thoracic kyphosis
As an attempt to balance in the sagittal plane.
Cerebral palsy
Less common than scoliosis; coxa valga.
Abnormal brain MRI.
Pseudoachondroplastic dysplasia and other dysplasias
May show hyperlordosis.
Table 4.97 Abnormally straight vertebral column (on lateral view)
Diagnosis
Findings
Comments
Straight back configuration; straight back syndrome
Absence of normal physiologic thoracic kyphosis in conjunction with decreased sagittal diameter of the thorax. Heart and great vessels may appear enlarged on the front view, with heart displaced to the left. Pectus excavatum accentuates the changes even more.
This configuration, or else pectus excavatum alone, is seen in about half of teenagers receiving chest radiographs for chest pain (thus straight back “syndrome”). Many persons with this configuration or with pectus excavatum can be shown to have mitral valve prolapse on sonogram.
Absence of cervical lordosis
Not a rare but a presumably normal finding in childhood.
Also common: pseudosubluxation between C2 and C3, and less often between C3 and C4.
Reflex pain, induced stiff back
Loss of cervical or lumbar lordosis due to pain-induced muscle spasm.
Fig. 4.259 Straight back configuration (syndrome, if associated with chest pain) in a 14-year-old girl. Total absence of thoracic kyphosis, yielding a narrowed thorax in midline.
Only gold members can continue reading. Log In or Register to continue