The Pediatric Vertebral Column: Anomalies of Vertebral Body Shape and Size
10.1055/b-0034-87913
The Pediatric Vertebral Column: Anomalies of Vertebral Body Shape and Size
Decreased Height
Generalized of Multiple Flattened Vertebrae (Platyspondyly)
In all cases of platyspondyly, it should be ascertained whether the dens is hypoplastic. A short dens predisposes to the dangerous atlantoaxial subluxation, particularly during sudden flexion or extension of the cervical spine (see, for example, Fig. 4.200).
Short rectangular vertebral bodies with vertically widened disk spaces, lumbar lordosis, and acute lumbar sacral angle anteroinferiorly. Narrowing of the distal lumbar spinal canal on the AP projection.
Short stature with short extremities and typical changes of the bony pelvis. Ice cream scoop en face proximal femurs in infancy. Occasional symptoms from narrow cervical spinal canal.
Universal striking platyspondyly, much more severe than achondroplasia.
Vertebrae appear like an “H” or a “U” on the frontal projection. European landline telephone receiver–shaped femora.
A member of the achondroplasia family, with much more severe enchondral slowing. This dysplasia, as implied by its name, is lethal. Survival can occur in the Torrance variant of thanatophoric dysplasia (straight femora).
Relatively mild platyspondyly. Short long bones, some bowed, and ribs (often only 11 pairs).
Severe rhizomelic shortening, may have camptodactyly.
Hallermann-Streiff syndrome
Narrow long bones and thin calvarium; multiple wormian bones.
Oculomandibulofacial syndrome.
Osteoglophonic dysplasia
Multiple fibrous metaphyseal defects; platyspondyly with anterior projection; acromelic shortening.
Craniofacial dysostosis with fibrous metaphyseal defects.
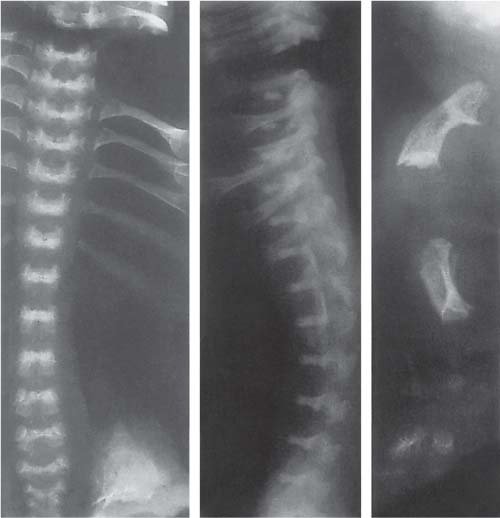
Fig. 4.193 Achondroplasia in a neonate. Lateral vertebral column: small vertebral bodies, widened intervertebral soft-tissue density spaces, thoracolumbar kyphosis, and sharply angled lumbosacral lordosis.Fig. 4.194 Thanatophoric dysplasia in a neonate with marked short stature on postmortem radiographs: striking platyspondyly, short ribs, European telephone receiver–shape of the femur, and rhizomelia.Fig. 4.195 Hypothyroidism in a neonate with rectangular small vertebral bodies and widened intervertebral soft-tissue density spaces. Hooklike anterior projection from the lower surface of L2 and L3 (arrows). Prominent soft-tissue density synchondrosis cleft between neural arches and the bodies. Striking Hahn vascular notches on midanterior bodies (courtesy of K. Koslowski, Sydney, Australia).
Generalized demineralization of bone with preservation of the cartilaginous zones of provisional calcification, including vertebral end plates (so that they are more conspicuous than normal). Multiple pathologic compression fractures. Thoracic vertebrae become flattened or anteriorly wedged; codfish (biconcave) vertebral deformity predominantly in the lumber region.
Many causes including steroid or heparin therapy, Cushing syndrome, idiopathic, sickle cell and other chronic anemias, leukemia, neuromuscular disease such as Duchenne muscular dystrophy, and homo-cystinuria.
If rickets is also present, the vertebral end plates (zones of provisional calcification) become difficult to see, which is the opposite of the situation in osteoporosis.
May also be a manifestation of renal osteodystrophy.
Anterior midbody tonguelike projections off the lumbar vertebrae, hypoplastic dens.
MPS IV. Pectus carinatum. Increased urinary keratan sulfate. Spinal cord may become severely damaged from atlantoaxial subluxation related to the short dens. Normal or high intelligence.
Other MPS and heteroglycanoses
In most types, such as Hurler and Hunter syndromes, there is an anteroinferior beaklike projection from lower thoracic or upper lumber vertebrae.
The vertebral change resembles hypothyroidism. Skeletal changes are more pronounced in MPS I–H, i.e., Hurler syndrome. Diagnostic findings in urine help s eparate the types. Also includes most mucolipidoses.
Multiple flattened vertebral bodies with irregular end plates. Coronal clefts in the midposterior vertebral bodies (common), spinal stenosis, kyphoscoliosis.
Spondyloepimetaphyseal dysplasia with widened metaphyses. Stiff, thickened joints. Myopia, deafness.
Vertebrae are biconvex in neonates; later diminished height with anterior wedging. End plates are irregular, as are epiphyses. Kyphoscoliosis.
A spondyloepiphyseal dysplasia. Short extremities including hands and feet.
Stickler syndrome (arthro-ophthalmopathy)
Significantly low vertebral body height.
Marfan-like body habitus, progressive myopia, and retinal detachment. Epiphyseal dysplasia. Early onset of arthritis.
Dysosteosclerosis
Platyspondyly and osteosclerosis (punctate margins of vertebral bodies). Resorption of phalangeal tufts.
Multiple fractures.
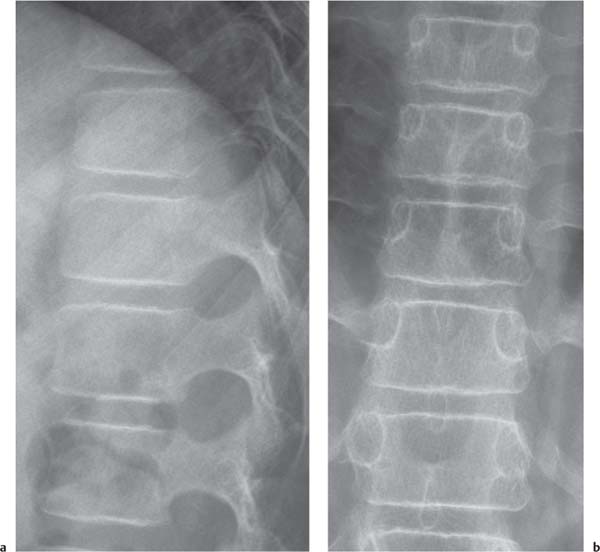
Fig. 4.196 Osteoporosis in a 13-year-old girl due to long-term steroid therapy for renal disease with simultaneously decreased body height and codfish vertebral shape. The end plates (zones of provisional calcification) maintain normal mineralization, and so appear strikingly dense compared to adjacent osteoporotic bone.Fig. 4.197a, b Osteoporosis in 10-year-old boy with Duchenne muscular dystrophy. Lateral (a) and frontal (b) images show the osteoporosis pattern of demineralized bone leaving the normal density zones of provisional calcification (end plates) highly conspicuous. Pedicle cortices en face (b) are thin.Fig. 4.198a, b Hyperparathyroidism, secondary to rickets in a 1-year-old child. Lateral (a) and frontal (b) images show the hyperparathyroidism and rickets pattern in contrast to Fig. 4.197. Because of the rickets, the end plates are quite inconspicuous as they are uncalcified. The pedicle cortices en face (b) are not thinned, but are somewhat washed-out, which is characteristic of hyperparathyroidism.Fig. 4.199 Morquio syndrome. Irregular loss of height of vertebral body with tonguelike center anterior projection (arrow) in a 2.5-year-old girl.Fig. 4.200a, b Atlantoaxial subluxation in Morquio syndrome in same patient as in Fig. 4.198. Cervical vertebral platyspondyly with short dens (D). The tip of the dens lies far below the anterior arch of C1 (arrowheads). (a) High position of the anterior arch of C1, in flexion. (b) Considerable atlantoaxial subluxation with (gentle) neck extension.Fig. 4.201 Spondyloepiphyseal dysplasia tarda. The vertebral bodies are narrow anteriorly (to viewer’s right) and biconvex posteriorly (“donkey back and belly” pattern).Fig. 4.202 Progressive pseudorheumatoid dysplasia. In this 13-year-old girl, some of the typical deformed lower thoracic and upper lumbar vertebral bodies are noted (here, there is excessive convexity of the upper and lower posterior body with tapered anterior portions).Fig. 4.203 Spondylometaphyseal dysplasia, Kozlowski type, showing short and sagittally elongated vertebral bodies.Fig. 4.204 Kniest disease. Short, sagittally long lumbar vertebral bodies with wavy upper and lower end plates and coronal cleft in L4 and forme fruste cleft in L3.Fig. 4.205 Dyggve-Melchior-Clausen dysplasia. Vertebral bodies with anterior and posterior humps (“Bactrian camel back”) of upper and lower margins; notches between the humps are concave toward the disks.Fig. 4.206 Pseudoachondroplasia. The bodies have diminished height, and the end plates are irregular. Diminished height is most pronounced anteriorly.
Loss of Height in Single or Multiple Vertebral Bodies
Table 4.66 Loss of height in single or multiple vertebral bodies
The most common cause of decreased vertebral height with destruction in childhood. Early radiographic changes: decreased disk space and destruction of the adjacent end plate, with possible posterior displacement of vertebral body. Earlier positive findings on MRI or NM. Later, occasionally wedging or fusion in the healing phase.
Rarely, central osteomyelitis in the vertebral body without disk space involvement.
Pyogenic bacteria, tuberculosis (starts anteri-orly), brucellosis (also starts anteriorly). Also often no organism found. Differentiation from tuberculosis in early phase may be difficult; there is later calcification and gibbus formation in tuberculosis.
Many involve more than one vertebral body. Anterior wedging with decreased height (exception: a Chance fracture is transverse through body and arch, which may lead to “taller” vertebra). May be a nose-shaped projection from an anterior corner. Dense callus seen within the bone after 10 d. Disk spaces are maintained.
Caution: Lateral compression on frontal projection may be subtle. CT and MRI are indicated in comminuted fractures for position of fragments and spinal cord involvement, respectively.
Child abuse
Often fractures are multiple; spinous processes alone may be fractured. Many other typical fractures elsewhere in skeleton.
On chest images, look for paraspinal hematoma or rib fractures.
Initial slight flattening, finally becoming vertebra plana. May affect single or multiple vertebral bodies. Arch elements less often affected; disk spaces intact. Regains height after the process is no longer active (the end plate zone of provisional calcification continues its enchondral bone growth).
Additional foci may be sought by bone scintigraphy, or, indeed, by PET scan. Typically painless in early stage.
Leukemia
Osteoporosis, pathologic compression fractures. Disk spaces maintained.
Osteoporosis and vertebral compression can be the presenting findings of leukemia (may even simulate child abuse).
Destruction and loss of height of one or more vertebral bodies. Disk spaces preserved. Pedicle destruction may occur.
Metastases: especially neuroblastoma (may be painless at first), rarely rhabdomyosarcoma, Wilms tumor, or Ewing sarcoma. Primary: Ewing sarcoma, may be sclerotic; vertebral body aneurysmal bone cyst, lucent and may collapse.
Chronic recurrent multifocal osteomyelitis
Associated sternal, clavicle, or long bone lesions.
May have acne or plantopalmar pustulosis (SAPHO [s ynovitis, a cne, p almoplantar pustulosis, h yperostosis, and o steitis] association). Many plasma cells but no organism on biopsy.
Fungal infection
Vertebral body destruction without disk space decrease.
When vertebral body is affected, the anterior body typically loses height sooner than the posterior.
Tubercuosis: skin testing; brucellosis: contact with affected livestock.
Thalassemia major; Gaucher disease
Single vertebra can be affected.
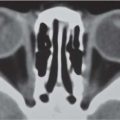
Fig. 4.207a–d Osteomyelitis. (a) “Pioneer” bone scintigraphy shows increased activity at L2 and L3 (arrows). Radiograph at that time was normal. (b) Three weeks later, there is loss of height of the L2-L3 disk space (arrow). The adjacent end plates no longer show normal calcification. (c) A different patient with more advanced disease. CT shows destruction in the L3 body with no involvement of spinal canal (arrowhead). (d) Coronal reconstruction of (c) showing downward extension of the defect into the body and narrowing of the disk space.Fig. 4.208 Wedge-shaped compression fractures of the thoracic spine (tomogram). Arrow points out the beaklike projection.Fig. 4.209 Langerhans cell histiocytosis. Flattened vertebral body L2 with maintained disk spaces. One cervical body was also affected in this nearly 1-year-old boy.Fig. 4.210 Fibrous dysplasia. Severe disturbance of vertebral column with S-shaped scoliosis and the deformed bodies have some loss of height.Fig. 4.211 Metastasis from Wilms tumor. Bowed downward depression of the upper end plate of a single vertebral body (initially unrecognized).Fig. 4.212a, b Tuberculosis. (a) Considerable loss of height of L3 body, with characteristic greater severity anteriorly. Loss of definition of upper end plate of L3 and part of lower end plate of L2. (b) Overall, the loss of height is greater on the left in this case.
True or Apparent Enlargement of the Vertebral Bodies
A compensatory increase in height occurs in vertebrae adjacent to a hemivertebra, acquired fused vertebrae after spondylitis, and in surgical posterior fusion in several types of scoliosis.
Table 4.67 Enlargement of the vertebral bodies
Diagnosis
Findings
Comments
Nonambulatory in early childhood: CNS impairment and neuromuscular disease
Hox gene dependent increased height adjacent to hemivertebra
Although tilted, the disk height tends to be normal. Bodies adjacent to butterfly vertebrae similar have medial lengthening in compensation.
May be a part of VATER association.
Caudal regression syndrome
Sacral aplasia; may have vertical overgrowth of remaining lumber bodies.
May be associated with maternal diabetes.
Rachischisis
Vertebral bodies may be enlarged on frontal view; disk spaces decreased.
Spina bifida aperta, perhaps with associated Chiari type II malformation.
Scheuermann disease
At the kyphosis, bodies may have increased sagittal and coronal width, along with reduced height especially anteriorly.
Often familial.
Compression fracture
Enlargement can occur in width sagittally or coronally; callus after 10 d.
MRI for associated cord damage.
Mass in the spinal canal
Apparent increase in height on lateral image is caused by narrowing in the sagittal dimension.
MRI to show the mass.
Tumors and metastases; aneurysmal bone cyst
Vertebral elements may be expanded by tumor growth or else diminished by pathologic fracture or collapse.
Hemangioma, lymphangioma, giant cell tumor, osteoblastoma, and renal cell carcinoma are possibilities.
Fig. 4.213 Nonambulatory, with relatively tall lumbar vertebrae. A severely brain damaged 8-year-old child with motor delay. There is no vertical stress on the spine. There is an incidental striking posterior vascular fissure in L3 (arrow).Fig. 4.214 Albright syndrome. In contrast to Fig. 4.209, the lumbar bodies may be relatively tall.
Table 4.68 Rarer syndromes with tall appearing vertebral bodies
Diagnosis
Findings
Comments
Pycnodysostosis
Relatively tall vertebral bodies. Bones abnormally dense and somewhat fragile.
Multiple wormian bones; obtuse angle of the mandible.