- 1
The _____________ costophrenic angle is deepest.
- A.
anterior
- B.
posterior
- C.
lateral
|
|
It is seen only on the lateral radiograph. It is not visible on the posteroanterior (PA) radiograph because the dome of the diaphragm is _____________ it.
- A.
above
- B.
below
- C.
posterior to
- D.
lateral to
|
|
On the PA view, fluid is best detected in the _____________ costophrenic angles.
- A.
anterior
- B.
lateral
- C.
posterior
- D.
medial
|
|
- 2
Romeo, shown in Figures 11-1B and 11-1C , slammed the back door just as the husband fired. The bullet, almost spent, just penetrated his chest wall and dropped harmlessly into the pleural space.
|
|
Figures 11-1B and 11-1C illustrate the depth of the _____________ costophrenic angles and the hazards of sex.
- A.
anterior
- B.
lateral
- C.
posterior
- D.
medial
|
|
(Editor’s note: Things were simpler in Dr. Felson’s time.) |
|
In Figure 11-1B (upright), the bullet in the posterior costophrenic angle appears to lie in the abdomen. In Figure 11-1C (lateral), the bullet is clearly in the posterior costophrenic angle. In Figure 11-1D (supine), several days later, the intrapleural bullet has shifted. |
- 3
Free pleural fluid (e.g., blood, exudate, transudate) is heavier than the air-filled lung and sinks to the base of the pleural cavity in the _____________ position.
|
|
It causes the normally deep _____________ and _____________ costophrenic angles to appear shallow or blunted.
- A.
anterior
- B.
lateral
- C.
posterior
- D.
medial
|
|
In Figure 11-2A (arrow), the lateral costophrenic sulcus is normal. In Figure 11-2B (arrow), the lateral costophrenic angle is _____________ because of a small effusion.
- A.
acute
- B.
shallow
- C.
round
|
|
Additional fluid tracks up the pleural space, forming a meniscus, as shown in Figure 11-2C (arrow). Figures 11-2A, 11-2B, and 11-2C are all the same patient. |
|
- 4
On the lateral x-ray, the signs are exactly the same. In Figure 11-3A (arrows), both costophrenic angles are _____________.
- A.
acute
- B.
shallow
- C.
round
|
|
In Figure 11-3B (lower arrow), the left costophrenic sulcus is _____________.
- A.
acute
- B.
shallow
- C.
round
|
|
In Figure 11-3C , fluid forms a meniscus, posteriorly ( arrowhead ). Pleural fluid is often seen tracking up the major fissure on the lateral examination, a helpful secondary sign of pleural effusion, Figure 11-3B, 11-3C (upper arrows). |
|
- 5
In Figure 11-3C , the _____________ diaphragm is not visible.
|
|
Why? This is a variation on the _____________.
- A.
air bronchogram
- B.
meniscus sign
- C.
silhouette sign
|
- C.
silhouette sign
The right contacts air in lung while the left contacts pleural fluid.
|
CLINICAL PEARL: The lateral film is more sensitive than the PA film for the detection of small effusions. If there is a discrepancy between them, believe the lateral. Figure 11-2 and Figure 11-3 are of the same patient. Compare each set of PA and lateral examinations. |
In Figure 11-4A , the apparent elevation of the left hemidiaphragm is actually subpulmonic fluid. The true diaphragm lies in normal position, but is obscured by a parallel layer of free fluid that often collects between the lung base and the top of the diaphragm. This “subpulmonic effusion” makes the “diaphragm” appear elevated. |
- 6
As you get older, gravity is less and less a friend. In radiology, however, gravity can be a friend.
|
|
What view would be most helpful in proving that Figure 11-4A has a subpulmonic effusion? _____________.
- A.
right lateral decubitus
- B.
left lateral decubitus
- C.
supine
- D.
oblique
|
- B.
left lateral decubitus
|
Figure 11-4B is a left lateral decubitus view of the patient shown in Figure 11-4A . The free fluid has redistributed to the dependent side of the left pleural cavity, between the lung and chest wall. Figure 11-4C , a computed tomography (CT) scan, shows a gravity-dependent pleural effusion layered posteriorly (E). In Figure 11-4D , ultrasound shows a free subpulmonic effusion (E) ( arrow = diaphragm). |
To discourage thieves, the farmer posted a sign: “Caution, one of these cabbages has been poisoned.” The next morning, he found the sign had been changed to read, “Caution, two of these cabbages have been poisoned.” |
- 7
We are now faced with the practical problem of recognizing subpulmonic fluid because it so closely simulates a(n) _____________.
- A.
pneumothorax
- B.
pneumonia
- C.
meniscus
- D.
elevated hemidiaphragm
|
- 7
D. elevated hemidiaphragm
|
On the left, the stomach bubble is normally separated from the lung base by only the thin diaphragm. Figure 11-5 shows the normal distance between the stomach and the lung ( arrow ). |
|
In Figure 11-6A , with left subpulmonic fluid, the gas bubble lies _____________ the lung base.
- A.
farther from
- B.
closer to
- C.
lateral to
|
|
This is known as the “stomach bubble sign.” |
|
There is no stomach bubble on the right. We often have to rely on the change of shape of the right “diaphragm” to diagnose subpulmonic effusion. In Figure 11-5 , the apex of each diaphragm is in the midclavicular line. With subpulmonic effusion, often the apex of the “diaphragm” moves to a more lateral position or changes shape, helpful signs of subpulmonic effusion on either side. |
- 8
Compare Figures 11-5 and 11-6A .
|
|
In Figure 11-6A , the left costophrenic angle is sharp but a _____________ tells us there is a left effusion.
- A.
hazy diaphragm
- B.
silhouette sign
- C.
meniscus
- D.
stomach bubble sign
|
|
What are the signs of pleural effusion on the right? _____________ and _____________
- A.
blunt costophrenic angle
- B.
stomach bubble
- C.
diaphragm changes shape
|
- A.
blunt costophrenic angle
- C.
diaphragm changes shape
|
In Figure 11-6B , the lateral x-ray shows blunting of both costophrenic angles posteriorly and a stomach bubble sign. There is also fluid in a major fissure ( arrow ). |
- 9
With a subpulmonic effusion:
|
|
The “diaphragm” may appear elevated.
|
|
The apex of the “diaphragm” usually shifts medially.
|
|
The costophrenic angle may be shallow or show a meniscus.
|
|
The stomach bubble should be seen adjacent to the lung base.
|
|
- 10
In the anteroposterior supine position, the fluid gravitates _____________.
- A.
anteriorly
- B.
posteriorly
- C.
laterally
|
|
It causes the affected hemithorax to appear _____________ or _____________.
- A.
more radiodense
- B.
less radiodense
- C.
more radiolucent
- D.
less radiolucent
|
- A.
more radiodense
- D.
less radiolucent
|
The supine patient in Figure 11-7A has _____________ pleural effusion.
- A.
a left
- B.
a right
- C.
a bilateral
|
|
The supine view is _____________ sensitive than the erect view in detecting effusion.
|
|
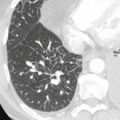
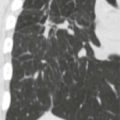
Figures 11-7B Shows a parasagittal CT with fluid layering posteriorly and in the major fissure (arrow). |
CLINICAL PEARL: Every student wants to know how much fluid one can see on a radiograph. The erect PA requires greater than 175 mL; the erect lateral, 75 mL; the decubitus, greater than 5 mL; the supine, more than several hundred milliliters. Now you know. (Does the name Pavlov ring a bell?) |
- 11
If one hemithorax is totally opaque, it may be due to _____________.
- A.
consolidation or atelectasis
- B.
a large pleural effusion
- C.
either
- D.
neither
|
|
If the “white lung” is due to atelectasis, the mediastinum shifts _____________ the lesion.
|
- A.
toward (collapse pulls the mediastinum toward that side)
|
- 12
Compare the “white lungs” of Figures 11-8A and 11-8B .
|
|
In Figure 11-8A , the mediastinum is _____________.
- A.
midline
- B.
shifted to same side
- C.
shifted to opposite side
|
- C.
shifted to opposite side
|
This is due to _____________.
- A.
pleural effusion
- B.
atelectasis
- C.
both
- D.
neither
|
|
In Figure 11-8B , there is shift to the same side. This is due to _____________.
- A.
pleural effusion
- B.
atelectasis
- C.
both
- D.
neither
|
|
CLINICAL PEARL: If there is a “white hemithorax” but no shift, both atelectasis and effusion may be present. There is a balance between collapse and pleural fluid, or a tumor “anchors” the mediastinum, preventing a shift. |
- 13
Encapsulated (loculated) pleural effusion is attributable to pleural adhesions that preexisted or developed after the effusion. The fluid _____________ shift in the supine or decubitus position.
|
|
- 14
Loculated fluid may simulate lung disease. See Figure 11-9A , an example of loculated pleural fluid.
|
|
The borders of an encapsulation are generally _____________ toward the lung.
|
|
The margin forms an _____________ angle with the chest wall when seen in profile ( arrows ).
|
|
The loculated fluid has the same appearance on the erect x-ray ( Figure 11-9A ) and on the supine CT ( Figure 11-9B ). CT shows a second smaller posterior loculation. Compare this with the free effusion of Figure 11-4C . |
- 15
Occasionally, fluid accumulates in a fissure. It may look like a lung mass. Because it splits the fissure, this “pseudotumor” is often _____________ in shape.
- A.
lenticular
- B.
spherical
- C.
crescentic
|
|
- 16
Intrafissural effusion (“pseudotumor”) is bounded by visceral pleura on both sides and its margins appear _____________ when seen in profile (on edge).
|
|
The encapsulated effusion in the minor fissure should have sharp margins in _____________ view(s).
- A.
the PA
- B.
the lateral
- C.
both
- D.
neither
|
|
The margins of the “mass” in the major fissure should be sharp in _____________ views(s).
- A.
the PA
- B.
the lateral
- C.
both
- D.
neither
|
|
(Remember, the beam must be parallel to the fissure to see it.) |
|
Figures 11-10A and 11-10B show the minor fissure “pseudotumor” (A) has sharp margins in the PA and lateral. The two loculated collections in the major fissure (B and C) are completely sharp only in the lateral projection. On the frontal image, portions of the major fissure pseudotumors are indistinct. |
CLINICAL PEARL: “Pseudotumors” are most commonly encountered in congestive heart failure. As the congestive heart failure resolves, the loculated fluid disappears (“vanishing tumor”). |
- 17
Figure 11-11A shows _____________, _____________, and _____________.
- A.
“elevated right diaphragm”
- B.
right pleural meniscus
- C.
elevated left diaphragm
- D.
lateral pleural thickening
|
- 17
A. “elevated right diaphragm”
- B.
right pleural meniscus
- D.
lateral pleural thickening
|
Remember the old films are your friends. Figure 11-11B was an image from 3.5 years earlier. Since then _____________ and _____________.
- A.
the right effusion is stationary
- B.
the right effusion is smaller
- C.
the left effusion is stationary
- D.
the left effusion is gone
|
- B.
the right effusion is smaller
- D.
the left effusion is gone
|
A current CT ( Figure 11-11C ) shows the right collection is 32 Hounsfield units and there is a small calcification. Diagnosis: _____________.
- A.
mesothelioma
- B.
empyema
- C.
chest wall mass
- D.
chronic organized pleural effusion
|
- D.
chronic organized pleural effusion
|
Empyema and hemothorax often loculate and become fibrous with time if not drained. This one was due to tuberculosis empyema in childhood. Note the left pleural is so thin, we can’t see it. |
|
- 18
Air in the pleural space is _____________ radiolucent than the lung.
|
|
With a pneumothorax, the visceral pleura is seen as a thin white line between air in the lung and air in the pleural space. |
|
When the lung is consolidated, the pneumothorax appears as a(n) _____________ adjacent to the air in the pleural space.
|
|
Figure 11-12A shows the thin pleura on end between the pleural air and the aerated lung ( arrows ). Figure 11-12B shows the pleural air against the edge of the consolidated upper lobe ( arrow ). There are no lung markings in the air-filled pleural space. There is also air in the subcutaneous tissues ( arrowhead ). |
- 19
Supine, the air collects _____________ and _____________.
- A.
anteriorly
- B.
posteriorly
- C.
inferiorly
- D.
superiorly
|
- 19
A. anteriorly
- C.
inferiorly
The highest point in the supine thorax
|
Figure 11-13A shows air inferiorly along the diaphragm. Figure 11-13B shows the anterior air collection on CT. |
|
- 20
The supine film is _____________ sensitive than the erect film for detecting pneumothorax.
- A.
more
- B.
slightly less
- C.
markedly less
|
|
If the patient cannot sit or stand, the decubitus position may help. The side in question should be up ( Figure 11-13C ). |
|
CLINICAL PEARL: You cannot rely on a supine image to rule out a pneumothorax or hydrothorax. |
- 21
Occasionally, air enters the pleural space with each breath but cannot escape, increasing the intrapleural pressure.
|
|
The increased pressure _____________ the diaphragm and collapses the lung.
|
|
It also shifts the mediastinum _____________ the pneumothorax.
|
|
This is known as a tension pneumothorax. |
|
CLINICAL PEARL: Rapid decompression of a tension pneumothorax can be lifesaving. Learn the clinical signs so that you can suspect it, diagnose it, and treat it rapidly. Signs include sudden dyspnea, decreased unilateral breath sounds, and jugular venous distention. |
- 22
Figure 11-14 shows the right lung is _____________.
- A.
consolidated
- B.
fully inflated
- C.
partially collapsed
- D.
hypolucent
|
- 22
C. partially collapsed
|
The right diaphragm is _____________ the left.
- A.
higher than
- B.
equal to
- C.
lower than
|
- C.
lower than
It is normally higher than the left.
|
The mediastinum is _____________.
- A.
left of midline
- B.
right of midline
- C.
midline
|
|
You have just diagnosed a tension pneumothorax. |
|
- 23
Figures 11-15A and 11-15B show _____________.
- A.
pneumothorax
- B.
hydrothorax
- C.
hydropneumothorax
|
|
The tip off is the _____________.
- A.
silhouette sign
- B.
stomach bubble sign
- C.
mediastinal shift
- D.
air-fluid level
|
|
There is air and fluid in the left pleural space because the lung was removed to treat cancer. |
|
- 24
The extrapleural space is a potential space that lies between the rib cage and the pleural space.
|
|
Lesions that arise in structures within or bordering the extrapleural space (e.g., ribs, muscle, connective tissue) may lift the adjacent _____________ pleura and push it toward the lung.
|
|
A typical extrapleural lesion is convex with a _____________ interface with the lung.
|
|
It forms an _____________ angle with the chest wall when viewed in tangent.
|
|
Compare a focal intrapleural lesion (encapsulated fluid) (see Figure 11-9A ) and an extrapleural lesion ( Figure 11-16 ). Both can form an obtuse angle with the chest wall. |
|
Figure 11-16 illustrates an extrapleural lesion. The convex margin facing the lung is sharp, and the borders are tapered (obtuse angle with chest wall). The rib fractures ( arrowheads in Figure 11-16 ) indicate the extrapleural origin. If no rib lesion is visible, it may be difficult to separate an extrapleural lesion from loculated fluid. |
- 25
Cross-sectional imaging helps separate extrapleural from intrapleural lesions by eliminating overlap of structures.
|
|
Figure 11-17A , a computed radiograph (scout view), shows a mass that forms a(n) _____________ angle with the chest wall.
- A.
acute
- B.
obtuse
- C.
right
|
|
The CT scan in Figure 11-17B shows that this mass is _____________.
- A.
intrapleural
- B.
extrapleural
|
|
CLINICAL PEARL: Most extrapleural lesions are due to rib fractures (see Figure 11-16 ) or rib metastasis (see Figure 11-17B ). |