The Pulmonary Hila
W. Richard Webb
CHEST RADIOGRAPHS
In most cases, plain films are adequate for identifying large hilar masses. Small masses can be more difficult to detect because of variation in the radiographic appearances of the normal hila.
Nonetheless, careful evaluation of the hila on chest radiographs can often yield significant diagnostic information. Abnormalities may present as a change in hilar size or density, bronchial wall thickening or narrowing of the bronchial lumen, or an alteration in the hilar contours.
Normal Hilar Contours
Frontal Radiograph
On a frontal (posteroanterior [PA] or anteroposterior [AP]) radiograph, the hilar shadows primarily represent the silhouettes of the hilar pulmonary arteries. The left pulmonary artery is situated higher than the right, and consequently the left hilum appears higher than the right in 97% of cases; in the remainder, they are at the same level.
Right Hilum
The superior portion of the right hilum is made up of the medially located truncus anterior, the artery supplying most of the upper lobe, and the right superior pulmonary vein, which forms the lateral margin of the upper hilum (Fig. 6-1). The anterior segment bronchus of the right upper lobe (RUL) is visible in 80% of patients as a 4- to 5-mm ring shadow in the lateral aspect of the hilum, accompanied by an artery of similar size. The RUL bronchus is sometimes visible.
The lower aspect of the right hilum is made up of the interlobar or descending pulmonary artery laterally and the bronchus intermedius medially. The pulmonary artery should measure 16 mm or less in thickness lateral to the bronchus (approximately the diameter of a dime) in men and 15 mm or less in women. The interlobar artery tapers inferiorly as it branches, with its lateral aspect appearing straight or slightly convex. Branches of the interlobar artery and segmental bronchi may be seen in the inferior hilum. Occasionally the lower part of the interlobar artery appears rounded, mimicking a mass or enlarged lymph node. This is most commonly seen when lung volumes are low.
A shallow concave angle is formed at the point where the superior pulmonary vein crosses the interlobar pulmonary artery. This is termed the hilar angle (Fig. 6-1).
The right inferior pulmonary vein is located inferior and medial to the hilum, and does not contribute significantly to the hilar silhouette.
Left Hilum
The left pulmonary artery passes above the left main and upper lobe bronchus, gives off small upper lobe branches, and descends posterior and lateral to the left upper lobe (LUL) bronchus and lower lobe bronchus. The superior hilar shadow is made up of the superior aspect of the left pulmonary artery, superior pulmonary vein, and small arterial branches (Fig. 6-2). The anterior segmental bronchus of the LUL may be seen in the lateral hilum at this level. As on the right, the interlobar pulmonary artery tapers caudally, but it is less clearly seen and more difficult to measure than the right pulmonary artery. The left inferior pulmonary vein contributes little to the hilar shadow.
Lateral Radiograph
The right and left hilar shadows are superimposed on the lateral radiograph, but specific parts of the right and left hila can be seen (Figs. 6-3 and 6-4). Identification of the hilar bronchi should be the first step in analysis of the hila on lateral films.
Right Hilum
The location of the tracheal carina and therefore the origins of the main bronchi can be determined by following the tracheal air column inferiorly. The carina is located at the point the air column begins to taper (Fig. 6-3B).
Below this level, a thin line, termed the intermediate stem line, is at least partially visible in 95% of patients (see Fig. 6-3). This line may be 5 cm or more in length and
measures up to 3 mm in thickness. It corresponds superiorly to the posterior wall of the right main bronchus and more inferiorly to the posterior wall of the bronchus intermedius. The RUL bronchus is visible in 50% of patients as a rounded lucency anterior to the upper aspect of the intermediate stem line, but it is seldom seen well.
measures up to 3 mm in thickness. It corresponds superiorly to the posterior wall of the right main bronchus and more inferiorly to the posterior wall of the bronchus intermedius. The RUL bronchus is visible in 50% of patients as a rounded lucency anterior to the upper aspect of the intermediate stem line, but it is seldom seen well.
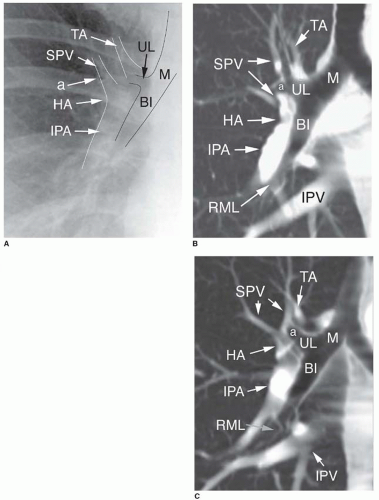 FIG. 6.1. Normal right hilum. A: Plain radiograph. The large bronchi (M, right main bronchus; UL, right upper lobe bronchus; BI, bronchus intermedius) are visible in the medial hilum. The anterior segment bronchus (a) is visible as a ring shadow lateral to the pulmonary arteries. Visible vascular structures include the apical branch of the truncus anterior (TA) in the medial superior hilum, and the superior pulmonary vein (SPV) in the lateral aspect of the superior hilum. The interlobar pulmonary artery (IPA) forms the lateral aspect of the inferior hilum and should measure 16 mm or less in men and 15 mm or less in women. A concavity is visible in the lateral hilum at the point the superior pulmonary vein crosses the interlobar pulmonary artery. This is termed the hilar angle (HA). B, C: Coronal CT reformations through the right hilum in two patients. In addition to the structures visible in A, the right middle lobe bronchus (RML) is visible inferiorly. The inferior pulmonary vein (IPV) lies medial and below the hilar shadow and is difficult to recognize on the chest radiograph because of the heart shadow. |
The anterior wall of the bronchus intermedius is visible as an edge, outlined by the right pulmonary artery and superior
pulmonary vein. In combination, these vessels create an oval shadow making up the anterior portion of the hilar silhouette. The right middle lobe bronchus is sometimes seen curving anteriorly below the inferior edge of this oval shadow. In 15% of individuals, the anterior wall of the RLL bronchus is visible below this level as a thin straight line, 1 to 2 cm long.
pulmonary vein. In combination, these vessels create an oval shadow making up the anterior portion of the hilar silhouette. The right middle lobe bronchus is sometimes seen curving anteriorly below the inferior edge of this oval shadow. In 15% of individuals, the anterior wall of the RLL bronchus is visible below this level as a thin straight line, 1 to 2 cm long.
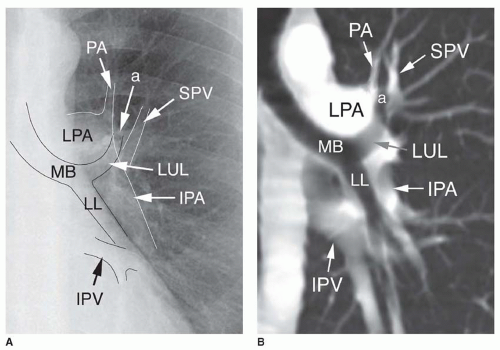 FIG. 6.2. Normal left hilum. A: PA radiograph. B: Coronal CT reformation. MB, left main bronchus; LUL, left upper lobe bronchus; LL, left lower lobe bronchus. The anterior segment bronchus (a) is visible as a ring shadow lateral to the main pulmonary artery, overlying the superior trunk of the left upper lobe bronchus. The left pulmonary artery (LPA) is visible as an oval opacity above the main and left upper lobe bronchus. The apical branch of the left pulmonary artery (PA) arises from the superior aspect of the pulmonary artery and as on the right is located medially. The superior pulmonary vein (SPV) forms the lateral aspect of the superior hilum. The interlobar pulmonary artery (IPA) forms the lateral aspect of the inferior hilum. The inferior pulmonary vein (IPV) may be visible inferiorly. |
Left Hilum
Below the carina, the left main bronchus is superimposed on the right main bronchus (see Fig. 6-4). A well-defined rounded lucency representing the horizontal portion of the distal left main bronchus and LUL (LM/LUL) bronchus is visible in 80% of subjects several centimeters below the carina. This lucency is more clearly seen, is larger, and is better defined than the rounded lucency representing the RUL bronchus because vessels surround much of its circumference. Localizing the LM/LUL bronchus is an important first step in identifying left hilar structures on the lateral radiograph. Because the left main bronchus is longer than the right, the LM/LUL bronchus is seen at a lower level than the RUL bronchus.
The anterior wall of the left lower lobe (LLL) bronchus is visible below the lucency of the LM/LUL bronchus as a thin curved line, concave anteriorly, in about 45% of cases. It arises tangential to the anterior wall of the LM/LUL bronchus.
The left pulmonary artery forms a comma-shaped opacity seen above the lucency of the LM/LUL bronchus and then passing posterior to it. Thus, while the right hilar vasculature largely accounts for the soft tissue in the anterior aspect of the combined hilar silhouette, the left pulmonary artery primarily accounts for its posterior aspect.
Plain Film Diagnosis of Hilar Mass or Lymphadenopathy
Frontal Radiograph
On a frontal radiograph, patients with a hilar mass or lymph node enlargement may show one of several findings:
Hilar enlargement (Fig. 6-5A)
A focal mass (see Fig. 6-5B)
Increase in hilar density (see Fig. 6-5C)
Hilar lobulation (see Fig. 6-5D)
Convexity of the hilar angle (see Fig. 6-5E)
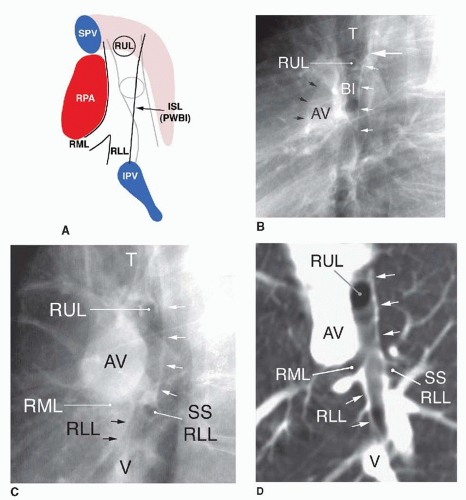 FIG. 6.3. Lateral chest radiograph; normal right hilar anatomy A: Diagram of right hilar structures. Anterior is to the left and posterior to the right. Right hilar structures appear dark and left hilar structures are dimmed. RUL, right upper lobe bronchus; BI, bronchus intermedius; RML, right middle lobe bronchus; RLL, right lower lobe bronchus; ISL, intermediate stem line; PWBI, posterior wall of bronchus intermedius. The interlobar right pulmonary artery (RPA) results in an oval shadow anterior to the BI. The superior pulmonary vein (SPV), along with the truncus anterior, forms the superior part of the vascular shadow anterior to the bronchi. The inferior pulmonary veins (IPV) are inferior. Left hilar structures are described in Figure 6-4A. B: Lateral radiograph showing right hilar anatomy. The trachea (T) is visible superiorly. The point at which the tracheal air column narrows (large white arrow) is the carina; the main and lobar bronchi are seen below this level. The right upper lobe bronchus (RUL) may be seen as a rounded lucency within the superior hilar shadow, slightly below the carina. Below the RUL, the bronchus intermedius (BI) is visible to the level of its bifurcation. The intermediate stem line or posterior wall of the bronchus intermedius is often visible as a thin white line (small white arrows). The oval shadow of the right hilar arteries and veins (black arrows; AV) is visible anterior to the bronchus intermedius. C: Lateral radiograph showing right hilar anatomy in a patient with left pneumonectomy. Only right hilar structures are visible. The trachea (T) is visible superiorly. Visible are the right upper lobe bronchus (RUL), intermediate stem line (posterior wall of the bronchus intermedius) (white arrows), right middle lobe bronchus (RML), superior segmental bronchus of the right lower lobe (SS RLL), and the anterior wall of the right lower lobe bronchus (arrows; RLL). Below the RUL, the bronchus intermedius (BI) is visible to the level of its bifurcation. The oval shadow of the right hilar arteries and veins (AV) is visible anterior to the bronchus intermedius, and the inferior pulmonary veins (V) are located inferiorly. D: CT reformation through the right hilum. RUL, right upper lobe bronchus; white arrows, intermediate stem line (posterior wall of the bronchus intermedius); RML, right middle lobe bronchus; SS RLL, superior segment bronchus of the right lower lobe; RLL, anterior wall of the right lower lobe bronchus; AV, right hilar arteries and veins; V, inferior pulmonary veins. |
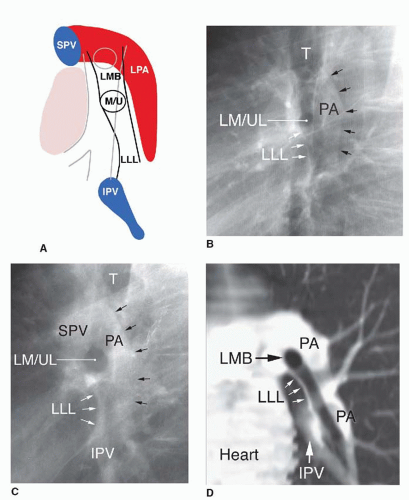 FIG. 6.4. Lateral chest radiograph; normal left hilar anatomy A: Diagram of hilar anatomy. Left hilar structures appear dark and right hilar structures are dimmed. LMB, left main bronchus; M/U, lucency of the left main and left upper lobe bronchus; LLL, left lower lobe bronchus; LPA, left pulmonary artery; IPV, inferior pulmonary veins; SPV, superior pulmonary vein. For right hilar structures see Figure 6-3A. B: Lateral radiograph showing left hilar anatomy; this is the same radiograph as in Figure 6-3B. The trachea (T) is visible superiorly. The horizontal portion of the left main and left upper lobe bronchus (LM/UL) results in an easily seen oval lucency. Above this level and superimposed on the bronchus intermedius, the main portion of the left main bronchus may be seen. The anterior wall of the left lower lobe bronchus (LLL) is visible below the LM/UL as a thin white line and typically appears concave anteriorly. PA, pulmonary artery. C: Lateral radiograph showing left hilar anatomy in a patient with a right pneumonectomy. Only left hilar structures are visible. The trachea (T) is visible superiorly. The oval lucency of the horizontal portion of the left main and left upper lobe bronchus (LM/UL) is easily seen. Below this level, the anterior wall of the left lower lobe (LLL) bronchus is visible as a thin white line, concave anteriorly. The left pulmonary artery (PA) is situated above and behind the LMB (black arrows). The left superior pulmonary veins (SPV) are visible anterior and superior to the LMB, and the inferior pulmonary veins (IPV) are located inferiorly. D: CT reformation through the left hilum. LMB, left main and left upper lobe bronchus; LLL, anterior wall of the left lower lobe bronchus; PA, left pulmonary artery; IPV, inferior pulmonary veins. |
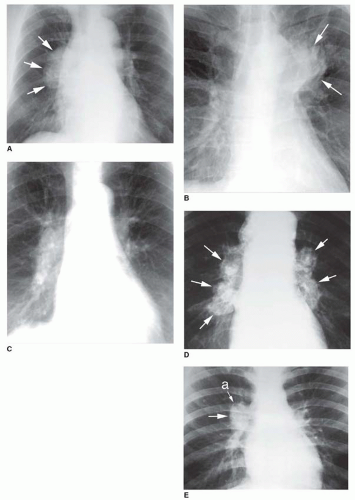 FIG. 6.5. Radiographic findings in hilar mass or lymph node enlargement. A: Hilar enlargement in a patient with lymph node enlargement due to metastatic renal cell carcinoma. The right hilum (arrows) is markedly enlarged and is rounded in contour, without its normal “vascular” shape. B: Focal hilar mass in bronchogenic carcinoma. A single, poorly marginated mass (arrows) obscures the upper left hilum. This appearance is typical of lung cancer originating in the hilum. C: Increase in hilar density due to right hilar carcinoma. The right hilum appears denser than the left. This is often due to mass or enlarged nodes anterior or posterior to the hilum. The right hilum is also enlarged, with a subtle convexity in the hilar angle. D: Hilar lobulation due to sarcoidosis. The hila have distinct lobulated contours (arrows) typical of lymph node enlargement. Node calcification is also seen. E: Convexity of the hilar angle in a patient with Castleman’s disease involving the right hilum. A mass (arrow) is visible in the region of the hilar angle. The mass projects lateral to the anterior segment bronchus (a) of the upper lobe. |
Hilar enlargement is often present in patients with hilar lymph node abnormalities (see Fig. 6-5A) or hilar mass (see Fig. 6-5B); it may be unilateral or bilateral. In the large majority of normal patients, the hila appear equal in size on frontal radiographs; comparison of the two hila is helpful in patients with a unilateral abnormality. Measurement of the width of the right hilum lateral to the bronchus intermedius may also be valuable in diagnosis; as indicated above, this measurement should be 16 mm or less in men and 15 mm or less in women.
Masses sometimes produce a unilateral increase in the hilar density on frontal radiographs (see Fig. 6-5A and C). This generally results when a mass or lymph node enlargement is located in the anterior or posterior hilum and is superimposed on the hilar shadow. In some patients, an increase in hilar density may be the only visible abnormality on the frontal radiograph; in such cases, the mass is often better seen on the lateral radiograph.
Hilar mass results in a focal alteration of the normal hilar contours. Lymph node enlargement may result in a focal abnormality or a more generalized lobulated appearance (see Fig. 6-5A and D). A common site for lymph node enlargement in the right hilum is the normally concave hilar angle; a convexity in this region is abnormal (see Fig. 6-5E).
The normal hila look vascular. The hilar shadows, primarily representing the pulmonary arteries, taper gradually with vessels arising from their periphery. Enlargement of a pulmonary artery results in increased hilar size and density, but the hilum retains its “vascular” appearance (Fig. 6-6). The appearance of pulmonary vessels converging on the lateral aspect of the hilum is termed the “hilum convergence” sign and is indicative of vascular dilatation as the cause of hilar enlargement. The hilar angle typically retains its normal concave appearance.
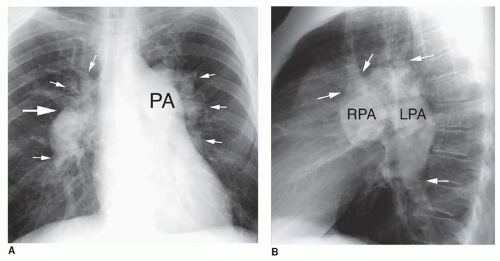 FIG. 6.6. Hilar enlargement in pulmonary hypertension. A: Enlargement of a pulmonary artery results in increased hilar size and density, but the hilum retains its “vascular” appearance. Vessels (small arrows) may be seen arising from the edges of the hilar shadow, the so-called hilum convergence sign, indicating the presence of vascular enlargement. The hilar angle (large arrow) remains concave. The main pulmonary artery (PA) is also enlarged. B: Lateral view. Although increased in size, the right (RPA) and left (LPA) pulmonary arteries retain their shape. Small branches arising from the edges of the arteries (arrows) result in the hilum convergence sign. (Figure continues.) |
Enlargement of hilar arteries is most typical of pulmonary hypertension. In addition to hilar enlargement, patients with pulmonary hypertension often show abnormal prominence of the main pulmonary artery on the PA radiograph and the main pulmonary artery and right ventricle on the lateral view. Pulmonic stenosis results in enlargement of the main and left pulmonary artery, while the right pulmonary artery usually appears normal in size.
Bronchial narrowing and obstruction associated with a hilar mass are usually difficult to diagnose on plain radiographs unless associated abnormalities such as mucous plugging, atelectasis, or obstructive pneumonia are visible (see Chapter 3).
Lateral Radiograph
Enlargement of the oval and comma-shaped shadows of the right and left pulmonary arteries indicates pulmonary artery dilatation (see Fig. 6-6B). As on the frontal radiograph, increased hilar size, focal mass, lobulation of hilar contours, or
alternation in the normal oval and comma-shaped shadows can indicate a hilar mass or lymph node enlargement.
alternation in the normal oval and comma-shaped shadows can indicate a hilar mass or lymph node enlargement.
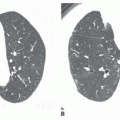
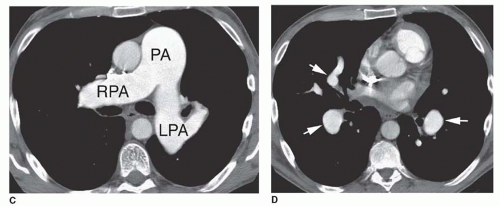 FIG. 6.6. (Continued.) C, D: CT shows enlargement of the main pulmonary artery (PA), right (RPA) and left (LPA) pulmonary arteries, and the interlobar and middle lobe branches (arrows). |
Attention to several specific regions visible on the lateral radiograph may also be helpful in diagnosis, including the posterior wall of the bronchus intermedius (PWBI), the inferior hilar window, and the RUL bronchus (sign).
Posterior Wall of the Bronchus Intermedius
The PWBI is seen as a vertical or slightly oblique line or stripe in about 95% of patients (see Fig. 6-3). At its upper extent, the PWBI is contiguous with the posterior wall of the right main bronchus, forming the intermediate stem line described above. This stripe is normally 0.5 to 3 mm thick. Thickening of this stripe may be seen in patients with neoplasm involving the hilum (Fig. 6-7), hilar adenopathy, interstitial pulmonary edema (Fig. 6-8), or interstitial thickening of various causes. Obliteration of the posterior bronchial wall and the presence of soft-tissue opacity behind it are virtually diagnostic of a mass in the hilum or adjacent lung.
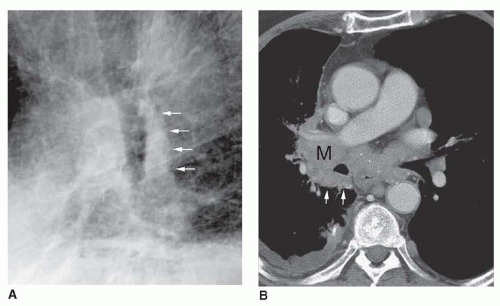 FIG. 6.7. Thickening of the posterior wall of the bronchus intermedius in right hilar carcinoma. A: Lateral chest radiograph shows marked thickening of the posterior wall of the bronchus intermedius (arrows). B: CT in this patient shows a right hilar mass (M) with infiltration and thickening of the posterior bronchial wall (arrows). |
Inferior Hilar Window
On the lateral radiograph, the oval soft-tissue shadow representing the right hilar vessels is visible in the anterior aspect of the silhouette of the superimposed hila, while the
comma-shaped left pulmonary artery occupies its superior and posterior aspect. The inferior hilar shadow contains no large vessels and consequently is termed the inferior hilar window (IHW). The IHW corresponds to an avascular region anterior to both lower lobe bronchi. It appears as a roughly triangular lucency in the anterior and inferior hilar shadow (Figs. 6-9).
comma-shaped left pulmonary artery occupies its superior and posterior aspect. The inferior hilar shadow contains no large vessels and consequently is termed the inferior hilar window (IHW). The IHW corresponds to an avascular region anterior to both lower lobe bronchi. It appears as a roughly triangular lucency in the anterior and inferior hilar shadow (Figs. 6-9).
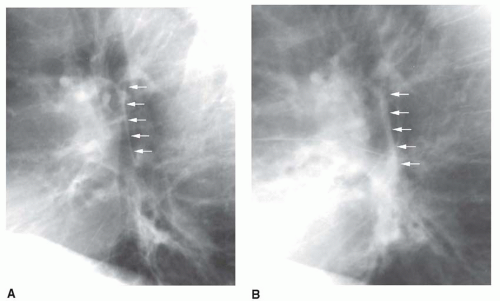 FIG. 6.8. Thickening of the posterior wall of the bronchus intermedius in pulmonary edema. A: A patient with longstanding renal failure shows a normal posterior bronchial wall (arrows). B: When the patient is in pulmonary edema, the posterior bronchial wall appears thickened (arrows). |
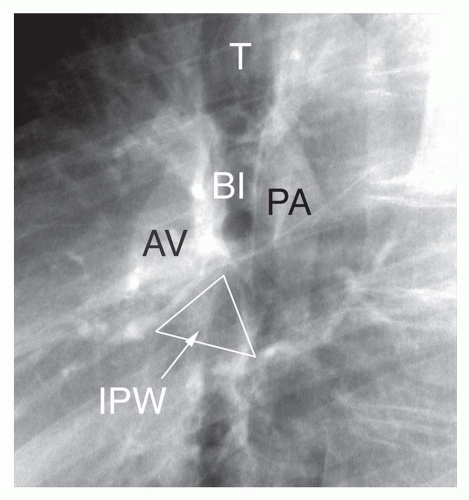 FIG. 6.9. The inferior hilar window. Lateral view. This image is the same as that in Figures 6-3B and 6-4B. The right hilar vessels (AV) occupy the anterior part of the hilar shadow. The left pulmonary artery (PA) is visible posteriorly and superiorly. The inferior hilar window is a roughly triangular lucency (IPW) in the anterior and inferior hilar shadow, below these major vascular branches. It represents an avascular region anterior to both lower lobe bronchi. T, trachea; BI, bronchus intermedius. |
In normal subjects, the inferior hilum appears radiolucent, and the composite hilar silhouette appears as an incomplete oval. The presence of a soft-tissue opacity of more than 1 cm in the IHW is more than 90% accurate in diagnosing a hilar mass or adenopathy in this region. In abnormals, the addition of an opacity in the inferior hilum (IHW) results in the appearance of a complete oval shadow on lateral radiographs
(Figs. 6-10 and 6-11). The side of the mass may be difficult to determine, although the frontal radiograph may help. Also, if a lower lobe bronchus is visible as a linear shadow, the mass must be on the opposite side.
(Figs. 6-10 and 6-11). The side of the mass may be difficult to determine, although the frontal radiograph may help. Also, if a lower lobe bronchus is visible as a linear shadow, the mass must be on the opposite side.
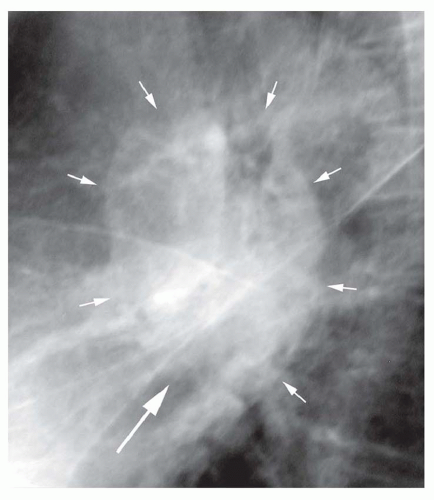 FIG. 6.10. Lymph node enlargement in sarcoidosis, with filling in of the inferior hilar window. Enlarged lymph nodes in the inferior hilar window (large arrow), when added to the shadows of the pulmonary arteries, result in a complete oval shadow on the lateral view (small arrows). This differs from the normal incomplete oval. |
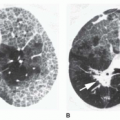
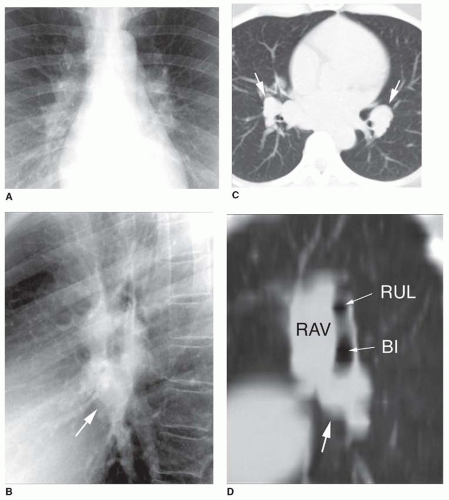 FIG. 6.11. Lymph node enlargement in sarcoidosis, with filling in of the inferior hilar window. A: PA chest radiograph shows subtle hilar lobulation. B: Lateral view shows lobulation of the hilar contours with filling in of the inferior hilar window (arrow). The hilar silhouette forms a complete oval. C: CT shows lymph node enlargement in the anterior inferior hila, in the space anterior to the lower lobe bronchi. D: CT reformation through the right hilum shows lymph node enlargement in the inferior hilar window (large arrow), inferior to the right hilar artery and vein (RAV). RUL, right upper lobe bronchus; BI, bronchus intermedius. |
Right Upper Lobe Bronchus (Sign)
Below the tracheal carina, two rounded radiolucencies are commonly seen, one above the other, in line with the tracheal air column and overlying the hilar bronchi. The lower of the two lucencies represents the horizontal portion of the left main and upper lobe bronchus. The upper lucency represents the RUL bronchus (see Fig. 6-3). It is usually less well seen, as it is not surrounded by vascular structures.
If the RUL bronchus is sharply marginated throughout its circumference (and more importantly if this represents a change compared to prior radiographs), hilar mass or adenopathy (surrounding and outlining the bronchus) is likely present (see Fig. 6-12). This sign can also be helpful in distinguishing hilar vascular enlargement (which does not result in this sign) from hilar node enlargement.
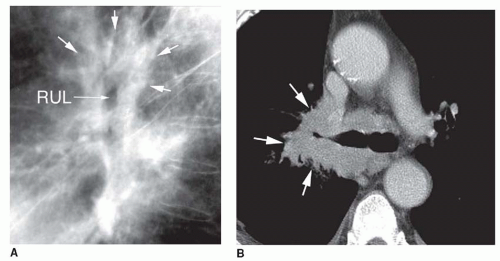 FIG. 6.12. Right upper lobe bronchus sign in lung cancer. A: Lateral radiograph shows the right upper lobe bronchus (RUL) as a lucency surrounded by mass (arrows). Thickening of the posterior wall of the bronchus intermedius is also visible. B: CT shows a large mass (arrows) surrounding the upper lobe bronchus. |
CT OF THE HILA
The pulmonary hila are complex structures containing the lobar and segmental bronchi, pulmonary arteries and veins, bronchial arteries and veins, soft tissue, and lymph nodes. The appearances of bronchi, vessels, and nodes and their consistent relationships at different hilar levels allow for reliable identification of these structures. Identification of specific bronchi is the first step in analysis of the hila. Bronchi are quite consistent in their branching pattern (Fig. 6-13).
CT of the Hilar Bronchi
Using a spiral CT technique and a slice thickness of 5 mm or less, all segmental bronchi should be visible. Their appearance depends on their orientation.
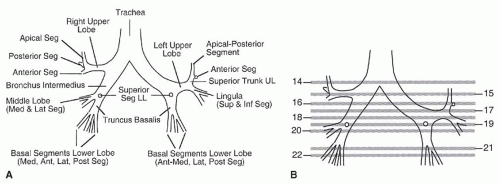 |
Bronchi oriented in or near the scan plane, and therefore seen along their axes as tubular structures, include the RUL bronchus (including both the anterior and posterior segmental bronchi), the LUL bronchus (including the anterior segmental bronchus), a portion of the middle lobe bronchus, and the superior segmental bronchi of both lower lobes.
Bronchi having a vertical course are seen in cross section and appear as circular lucencies. These include the apical segmental bronchus of the RUL, the apical-posterior segmental bronchus of the LUL, and proximal portions of both lower lobe bronchi (below the takeoff of the superior segmental bronchi), and the medial and posterior basal lower lobe segments.
The most difficult bronchi to visualize clearly are those oriented obliquely relative to the scan plane, including the superior and inferior lingular bronchi, the lateral and medial segmental bronchi of the middle lobe, and the anterior and
lateral basal lower lobe segments. Such bronchi appear elliptical on CT.
lateral basal lower lobe segments. Such bronchi appear elliptical on CT.
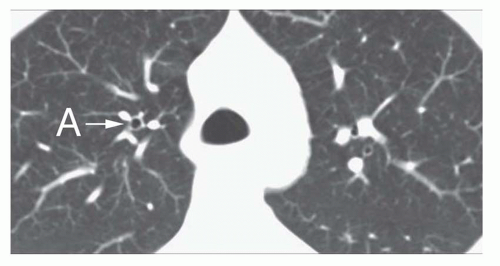 FIG. 6.14. Apical segment bronchus right upper lobe. The bronchus (A) is visible as a ring shadow at a level near the carina. A vessel of similar size and shape medial to the bronchus represents the artery to the apical segment. A vein characteristically lies lateral to the bronchus. |
Right Bronchial Anatomy
The right main bronchus is relatively short, dividing into the RUL bronchus and bronchus intermedius. Often the carina, right main bronchus, and RUL bronchus are visible on a single scan.
Right Upper Lobe Bronchus
The RUL bronchus is always found at or just below the carina. The RUL bronchus courses laterally for 1 to 2 cm before dividing into its three segmental branches (apical, anterior, and posterior; Figs. 6-14 and 6-15A). Characteristically, the posterior wall of the RUL bronchus is sharply outlined by lung and is seen as a thin line (see Fig. 6-15A). The upper limit of normal for thickness of the posterior wall of the RUL bronchus is 3 to 5 mm. However, the posterior part of the arch of the azygos vein can result in apparent bronchial wall thickening.
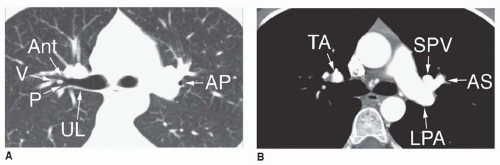 FIG. 6.15. Right upper lobe bronchus; apical posterior segment bronchus of left upper lobe. A: Lung window. On the right side, slightly below the carina, the right upper lobe bronchus (UL) is visible along its axis. Its posterior wall is visible as a thin white line. It branches in a Y shape into its anterior (Ant) and posterior (P) segments. On the left side, the apical posterior segment bronchus (AP) is visible as a ring shadow. B: Soft-tissue window scan following contrast enhancement. On the right, the truncus anterior (TA) lies anterior to the right upper lobe bronchus and appears similar in size to the main bronchus seen on the same scan. A vein lies between the anterior and posterior segmental bronchi (V in A.). On the left, the left pulmonary artery (LPA) is posterior. The artery supplying the anterior segment (AS) of the left upper lobe is located medial to the apical posterior segment bronchus. The superior pulmonary vein (SPV) is anterior and medial to the anterior segment artery.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|