Fig. 2.1
An old image showing the distribution of function in a normal thyroid gland measured with 131I
The clinical scene in nuclear medicine today is hybrid imaging. It is the modality developing most rapidly. By hybrid imaging a combination of two different modalities is meant, most commonly SPECT and computed tomography (CT) or PET and CT, resulting in a combination of molecular/biologic and structural information displayed in a fused mode (Fig. 2.2).
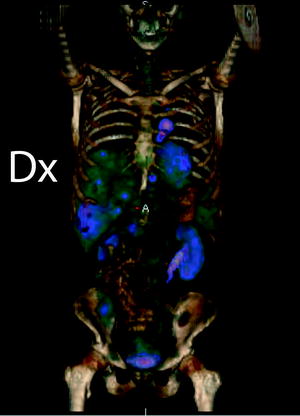
Fig. 2.2
An FDG-PET/CT 3D image of a patient with lung cancer. The skeleton is from the CT acquisition and the uptake in the liver, kidneys, bladder, heart and the lung tumour is from the PET acquisition
Hybrid systems with a combination of PET and magnetic resonance tomography (MR) are being introduced in the clinical setting, and greater details will be given in Chap. 4. The structural part, the CT, contributes with morphologic information but also with transmission data which is used for attenuation correction of the PET or SPECT data. The strengths of CT are the spatial resolution and the contrast [2, 3]. PET and SPECT on the contrary have a relatively low spatial resolution, and the strength is the very high molar sensitivity giving the possibility to examine small changes in physiology [4, 5]. A comparison of different imaging modalities is shown in Table 2.1. Also gadolinium-enhanced magnetic resonance imaging (Gd-MRI), which is not based on the use of ionizing radiation, is shown for comparison.
Table 2.1
Molar sensitivity and spatial resolution for different tomographic modalities
Modality | Concentration at target | Resolution (mm) |
|---|---|---|
PET | Picomolar (10−12) | 4–6 |
SPECT | Nanomolar (10−9) | 4–12 |
Gd-MRI | Milli-micromolar (10−3/−6) | <0.5 |
CE CT | Millimolar (10−3) | <0.5 |
Before an examination with radiation is done, it has to be justified. The appropriateness and the benefit versus risk have to be decided, and the examination procedure has always to be optimized. A radiopharmacon, usually consisting of a radionuclide bound to an active substance defining which function is examined, is needed. For SPECT studies the most common radionuclide is 99mTc, a pure gamma emitter and 6 h half-life (T 1/2). For PET the working horse is 18F, a positron emitter with 109 min T 1/2. The active substance can be a bone seeker, such as methyl-diphosphonate (MDP) for SPECT or fluro-2-deoxy-2-d-glucose (FDG), which measures the metabolism in PET. The radiopharmacon or tracer can be administered to the patient in different ways, of which intravenous (iv) injection is the most common.
Nuclear medicine covers a variety of clinical questions, and it is the clinical question deciding the setup of a nuclear medicine examination. Some examples of the most common and most recent applications of nuclear medicine imaging, listed according to the imaging modality, are presented in the following sections, and some indications on future trends and need, viewed from the medical perspective, are given in the end.
2.2 Gamma Camera and SPECT Imaging
Examination of the whole skeleton with 99mTc-MDP (methyl-diphosphonate) to diagnose metastases or other bone diseases is a very common examination with conventional gamma camera (Fig. 2.3). Bone scintigraphy has been the method of choice to follow patients with oncology diseases, but imaging with different tracers in PET/CT is rapidly developing [6–8].

Fig. 2.3
A whole body bone scintigram of a normal skeleton
By using a substance measuring the regional brain blood flow (rCBF), the brain function can be measured by a SPECT or a SPECT/CT camera [9, 10]. Hexamethylpropyleneamine oxime (HMPAO) or Neurolite is distributed in the brain in relation to the blood flow, and most of the uptake takes place during the first passage. The rational for examination is that brain function is correlated to blood flow. The examination is used to diagnose dementia and to differ between neurodegenerative and vascular dementias (Fig. 2.4a). The same substance (HMPAO) can also be used to label white blood cells and with that substance inflammatory or infectious diagnoses can be made. This is mostly used to diagnose inflammatory bowel disorders (Fig. 2.4b). Blood flow and myocardial function can be examined with other radiopharmaceuticals. A cocaine analogue, 123I-FP-CIT binding to dopaminergic neurons, is used to examine the function in striatum which is affected in parkinsonian diseases and Lewy body dementia, but not in essential tremor, making it possible to set correct diagnosis with high sensitivity and specificity (Fig. 2.5) [11–13]. If the patient is allowed to breathe an aerosol of carbon particles covered with 99mTc, the distribution of air in the lungs can be made.
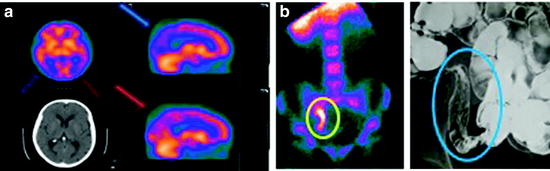
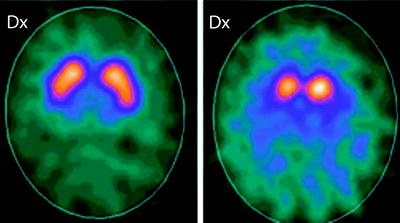
Fig. 2.4
(a) A CT and an rCBF-SPECT study with HMPAO of a patient with dementia. The blood flow is reduced in the parietal lobes bilateral (red and blue arrows). The CT shows no atrophy. (b) On the left, an intense uptake of HMPAO-labelled white blood cells is seen in the right fossa (in the yellow circle) in a patient under investigation of inflammatory bowel disease. The uptake is located to the bowel section with acute inflammation. On the right, the cobble stone appearance of the mucosa is visualized with the small bowel contrast examination
Fig. 2.5
FP-CIT-SPECT images of two patients with tremor. The one on the left has a normal dopamine transporter SPECT study with preserved activity in striatum bilateral and is suffering from essential tremor. The patient on the right has reduced activity in putamen bilateral (the lower part of striatum) and on the right nucleus caudatus consistent with a parkinsonian disease
This is used in combination with an iv injection of 99mTc-labelled macroaggregates of albumin, small enough to enter the capillaries. By measuring the ventilation and blood flow distribution in the lungs, pulmonary embolism can be diagnosed. A mismatch is seen in pulmonary embolism, with activity defect in the perfusion but not in the ventilation study (Fig. 2.6). Even if CT examination of suspected pulmonary emboli is the first choice of examination, there is a clinical need of scintigraphy studies [14, 15].
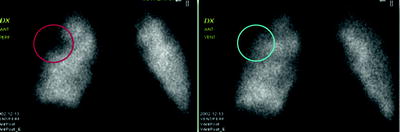
Fig. 2.6
Shows a perfusion and ventilation scintigraphy of a lung. To the left an image of a perfusion scintigraphy is seen. A triangular shaped region with reduced perfusion is seen in the upper lateral segment of the lung (red circle). To the right the ventilation scintigram of the same patient is shown. The ventilation in the entire lung is normal. The corresponding segment to that with reduced perfusion is delineated with a blue circle.
2.3 PET/CT Imaging
PET/CT was introduced to the clinical practice in the beginning of 2000 [16, 17] and after that a tremendous development has been taking place. Compared to SPECT, the PET scanner has a significantly higher sensitivity and a slightly better spatial resolution (Table 2.1). Instead of using gamma emitters, positron emitters are used. A positron emitter gives away a positron from the nucleus, and since this antiparticle cannot exist, it interacts with an electron and annihilation takes place. The result is that mass converts to energy, and 511 keV photons radiating almost 180° in opposite direction are produced. These 511 keV photons are measured by the PET-detectors and transformed into images, as described in Chaps.3 and 4. The invention of PET scanning is not new, and already in the 1950s, arsenic was used to image brain tumours [18].
The combination of PET and CT (PET/CT) is a molecular imaging modality allowing us to visualize different biochemical pathways in cancer cells. Imaging is usually done with 11C- or 18F-labelled tracers. The sensitivity is high, making it possible to detect picomolar and down to nanomolar concentrations of the tracer in vivo and thus to perform imaging using non-pharmacological concentrations of the substances. This counts also for SPECT and gamma camera imaging. Oncology diseases are still the major indication for PET/CT even if the use for cardiac, brain imaging and inflammation is increasing.
Initially, the CT examination was mainly restricted to attenuation correction and anatomical mapping to facilitate the localization of the PET uptake. Today, the vast majority of PET/CT scanners are equipped with a state-of-the-art CT, and an increasing proportion of PET/CT studies are made with high-quality diagnostic CT. This true hybrid imaging sets demands on the physicians to have qualification in both radiology and nuclear medicine to evaluate the entire hybrid examination. Collaboration between a radiologist and a nuclear medicine specialist making the evaluation together is another working strategy. Furthermore, the competence of the nurses/technicians is changing, and knowledge from both radiology and nuclear medicine is needed. The clinical routine to examine patients will also change with replacement from CT to PET/CT in an increasing proportion of, for example, lung cancer patients. In summary, the development and diffusion of hybrid imaging has increased the collaboration between radiology and nuclear medicine.
2.3.1 Fluoro-2-Deoxy-2-d-Glucose
The absolute most commonly used PET tracer for imaging is FDG labelled with 18F for oncologic diseases. The tracer is delivered by the blood and taken up by the tumour cells with help of glucose transporters. Inside the cell FDG is phosphorylated by hexokinase, and the product FDG-6P does not continue in the metabolic route. It remains entrapped in the tumour cell where it can be measured by the PET scanner. Therefore, this tracer acts as a surrogate marker for metabolism, and this pathway is the one which is most frequently imaged. FDG has been in use since 1978 [19], and its use is reimbursed for most solid tumours (Fig. 2.7).
Fig. 2.7
A schematic drawing of the FDG uptake and entrapment in tumour cells
PET/CT with FDG has a high impact in clinical handling, and in 2001, a study was published showing changed clinical management of approximately a third of patients with lung cancer, colorectal cancer, melanoma and lymphoma after adding FDG-PET for staging [20]. In two publications from 2008, the impact of PET/CT on expected management of patients with cancer was evaluated based on ~23,000 PET/CT studies. These papers also concluded major changes in patient handling in approximately one-third of patients with varying oncologic diagnosis. These changes affected clinical handling for diagnosis, initial staging, restaging as well as for suspected recurrence [21, 22]. As medicines become more and more personalized, PET/CT can be of help in staging, in treatment planning and in some diagnoses also in early treatment evaluation.
2.3.2 Lung Cancer
There is a strong evidence for the use of FDG-PET/CT in initial staging for lung cancer when curative treatment is intended [23–25]. Evaluation of lymph nodes in mediastinum has the highest added value. If lymph nodes are PET negative, spread disease can be ruled out. FDG-positive nodes on the contrary are recommended to be biopsied before final staging, due to the risk of false-positive findings in inflammation. The staging with PET/CT gives major information for the treatment decision and gives also an indication of prognosis for the patient. For lung cancer, FDG-PET/CT is furthermore recommended for radiation treatment planning in order to include all active disease and to avoid radiation of for instance lung atelectasis which can be impossible to delineate with CT [24, 26].
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


