|

Illustrate the normal gross and sectional anatomy of the scrotum and penis, including the vascular anatomy.
Describe the sonographic appearance of the normal scrotal and penile anatomy.
Explain the technique and protocol for sonographic evaluation of the scrotum and penis.
State the indications for a sonographic examination of the scrotum and penis.
Identify the common pathologic conditions that can result in an acute painful scrotum and penis.
Differentiate common extratesticular abnormalities from intratesticular abnormalities.
Describe the sonographic characteristics and laboratory values associated with scrotal masses.
Describe the sonographic characteristics associated with penile abnormalities.
alpha-fetoprotein levels are measured during pregnancy to detect certain fetal anomalies; blood levels may also be elevated with hepatocellular carcinoma and certain testicular cancers
human chorionic gonadotropin is produced during pregnancy and is also secreted by some malignant tumors, including certain testicular cancers
two cylindrical columns of spongy tissue running parallel dorsally that serve as the main erectile structures in the penis
single column of spongy tissue that contains the urethra and expands distally to form the glans penis; this tissue expands slightly during an erection but not to the extent of the cavernosa
undescended testicle—occurs when one or more of the testis fails to descend into the scrotum before birth
surgical procedure to remove a hydrocele
an increase in blood flow to the tissue
tissue death that occurs owing to a lack of blood flow
passage in the anterior abdominal wall in both females and males that transmits structures from the pelvis to the perineum
a surgical procedure done to fasten an undescended testicle into the scrotum or to repair an acute testicular torsion
a network of veins that drain the epididymis and testis; it is located in the spermatic cord and empties into the right and left testicular veins
characterized by fibrotic thickening of the tunica albuginea, resulting in the formation of fibrous plaques, which can lead to severe curvature of the penis and difficulty in achieving an erection
defined as a painful and prolonged penile erection, with or without stimulation
a sonographic indicator of an organ to perfusion; it is calculated from the peak systolic velocity and the end diastolic velocity of blood flow
scrotoliths or scrotal pearls are benign extra testicular macrocalcifications located within the scrotum, between the layers of the tunica vaginalis
process in which spermatozoa are produced
dense fibrous sheath that encapsulates and provides structure and support to the testicles and corpora of the penis
consists of forced expiration against a closed glottis after a full inspiration; the Valsalva maneuver increases the intra-abdominal pressure and is helpful in diagnosing a varicocele and scrotal hernia
surgical procedure in which the vas deferens is cut, tied, cauterized, or otherwise interrupted; the semen no longer contains sperm, preventing conception
a membranous sac attached to an embryo formed by cells adjacent to the embryonic disk
when evaluating large anatomic segments with inflammatory processes and fluid collections because a wider FOV provides a greater understanding of anatomical relationships10 (Fig. 19-2).
 FIGURE 19-1 Convex transducer. Transverse image of enlarged scrotum best seen with a convex probe. Note the large echogenic hydrocele compressing and displacing the testis (T). |
 FIGURE 19-2 Extended field of view (FOV). Longitudinal extended FOV image of the scrotum, including the testis and the epididymal head (H), body (B), and tail (T). |
Obtain power, color, and spectral Doppler tracings to confirm the presence or absence of intratesticular arterial and venous flow.
Grayscale images are often nonspecific for evaluating testicular torsion and often appear normal when torsion is acute.16
Spectral Doppler findings suggestive of partial torsion include asymmetry in resistive indices with decreased diastolic flow or diastolic flow reversal.16
In the clinical setting of epididymo-orchitis, when focal hypoechoic areas are detected within the testis, ultrasound follow-up is recommended after antibiotic treatment is completed to confirm the diagnosis and observe resolution, so that tumor and or infarction can be ruled out.7
Large hydroceles, hematomas, marked scrotal edema, and epididymo-orchitis are scrotal conditions that decrease intratesticular perfusion, mimicking testicular torsion.
In patients presenting with acute epididymo-orchitis, spectral Doppler demonstrates decreased vascular resistance (resistive index [RI] < 0.5) compared with the normal contralateral testis and epididymis.11
Reversal of the spectral diastolic component of the intratesticular arterial flow in patients with acute epididymo-orchitis suggests venous infarction.18
Use color and power Doppler to differentiate epididymitis from an enlarged, noninflammatory epididymis status postvasectomy.
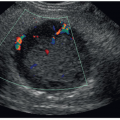
Because primary varicoceles may decompress when the patient is supine, perform the Valsalva maneuver or scan the patient in the upright position to increase venous blood flow.
Large varicoceles can extend posteriorly, lateral, and inferiorly to the testis, mimicking epididymitis.
The inguinal canal and abdomen are imaged when hernia, secondary varicocele, undescended testis, and or postsurgical complications are suspected.
Evaluate the spermatic cord to detect abnormalities such as solid masses, hematomas, abscess, torsion, hernias, and hydroceles.
Use a gel standoff pad to evaluate anterior and/or superficial lesions, such as those in the tunica vaginalis.
Longitudinal midline testis grayscale: Measure the length, and anteroposterior (AP) diameter. Midline testis: assess arterial and venous flow with color and/or power Doppler and color with spectral Doppler. Obtain an RI measurement of arterial flow.

FIGURE 19-3 Comparison. A: Transverse image of normal bilateral right (RT) and left (LT) testes (T) demonstrating similar homogeneous echogenicity. B: Transverse image of normal bilateral right (RT) and left (LT) testes (T) demonstrating normal flow bilaterally.

FIGURE 19-4 Schematic illustration of longitudinal scrotal anatomy and relevant adjacent structures. 1, spermatic cord; 2, head of epididymis; 3, testis superior; 4, testis—mid; 5, testis—inferior; 6, tail of epididymis. Note that the body of the epididymis is seen in sections 3, 4, and 5.

FIGURE 19-5 Schematic illustration of transverse scrotal anatomy and relevant adjacent structures. 1, spermatic cord; 2, head of epididymis; 3, testis—superior; 4, testis—mid; 5, testis—inferior; 6, tail of epididymis. The body of the epididymis is seen in sections 3, 4, and 5.
Measure the AP diameter of the scrotal wall. Subsequent images should include the lateral and medial portions of the testis.
Longitudinal “cine-clip” of testis lateral to medial.
Longitudinal epididymal head grayscale: Measure the AP diameter and length.
Longitudinal epididymal head with color and/or power Doppler to assess vascular perfusion.
Longitudinal epididymal body: The normal narrow body of the epididymis lies adjacent to the posterolateral margin of the testis. Measure the AP diameter. Perform color and/or power Doppler imaging to assess vascular perfusion.
Longitudinal inferior testis and epididymal tail: Measure the superior to inferior diameter of the epididymal tail. Use color and/or power Doppler to assess vascular perfusion.
Longitudinal spermatic cord grayscale at rest and with the Valsalva maneuver and with color and/or power Doppler, to assess venous reflux and increased flow: Measure the AP diameter of the largest vein(s) on the grayscale image.
Transverse superior testis with epididymal head in grayscale and color to assess vascularity of epididymis compared with the testis.
Transverse mid-testis: Obtain transverse measurement in grayscale, and document with color Doppler. Subsequent images should include inferior testis and inferior testis with epididymal tail. Obtain grayscale and color Doppler to assess the vascularity of the epididymis compared with the testis.
Measure the AP diameter of the scrotal wall.
Transverse “cine-clip” testis superior to inferior.
Transverse spermatic cord grayscale at rest and with the Valsalva maneuver, and with color and/or power Doppler: Measure the AP diameter of the largest vein on the grayscale image.
 FIGURE 19-6 Scrotal wall. Longitudinal image of normal scrotal wall thickness (calipers). |
with the testis.2,9,24,25 The narrow body and curved tail are smaller, more variable in position, usually posterior and inferior to the testis, and best evaluated in the longitudinal scan plane2,4,15,21,24,25 (Fig. 19-10B, C). Color flow imaging of the normal epididymis demonstrates speckled intraepididymal arterial flow7 (Fig. 19-10D).
 FIGURE 19-7 Spermatic cord. A: Longitudinal image of the normal spermatic cord (arrows). B: Transverse image of the normal spermatic cord (arrows) with sonolucent ducts and vessels. C: Longitudinal and transverse (D) images of the normal spermatic cord (arrows) with color flow at rest. Longitudinal (E) and transverse (F) images of the normal spermatic cord (arrows) with slightly increased venous flow during the Valsalva maneuver. |
 FIGURE 19-8 Ductus (vas) deferens. A: Longitudinal color Doppler image of the normal suprascrotal segment of the ductus (vas) deferens. Calipers measure the total AP thickness. Arrow represents the inner lumen of the duct. B: Transverse color Doppler image of the normal suprascrotal segment of the ductus (vas) deferens within the spermatic cord. Note the duct is avascular. Calipers measure the AP and transverse diameter. Arrow designating the “target” appearance. C: Longitudinal grayscale image of the normal ductus (vas) deferens, scrotal segment. Calipers measure the convoluted shaped duct arising from the tail of the epididymis, inferior to the testis (T). |
 FIGURE 19-9 Schematic illustration of the sagittal anatomic section of normal scrotum. |
scrotum.7 The scrotal ligament can be seen in the presence of a hydrocele. The sonographic appearance of the scrotal ligament is an echogenic band extending from the caudal end of the testis to the scrotal wall7 (Fig. 19-12).
 FIGURE 19-10 Epididymis. A: Longitudinal image of normal testis (T) and epididymal head (E). B: Longitudinal image of normal testis (T) with the body of epididymis (B). C: Longitudinal image of normal testis (T) and tail of epididymis (E). D: Longitudinal color image of testis (T) with normal flow in the epididymis (E). |
has been identified unilaterally in 34% and bilaterally in 12% in postmortem studies.10,14 The appendix epididymis is approximately the same size as the appendix testis.10,11 The shape of the appendix epididymis is more of a stalk-like structure.10,11 Appendages of the testis and epididymis are visualized sonographically as isoechoic to echogenic protuberances superior to the testis and epididymis.7,10,11,14 Occasionally, the appendix epididymis may swell or distend, forming a cyst-like structure, not to be confused with an epididymal cyst10 (Fig. 19-16D).
 FIGURE 19-11 Postvasectomy changes. A: Longitudinal color Doppler image of enlarged avascular heterogeneous epididymal body (EB) (arrows) in a postvasectomy patient. Normal testis (T). B: Longitudinal image of scrotum demonstrating multiple large spermatoceles (S) of the head and body of epididymis. C: Longitudinal image of testis showing cystic changes of dilated rete testis (RT). D: Longitudinal image of diffusely enlarged hypoechoic epididymis with sperm granulomas (SG). Normal testis (T). E: Transverse power Doppler image of a sperm granuloma (arrows) with intravascular flow, within the tail of the epididymis (ET) postvasectomy. F: Longitudinal image of an enlarged “painful” ductus (vas) deferens (arrows) suprascrotal segment, with an echogenic “Clip Artifact” (large arrow) postvasectomy. G: Longitudinal image of a sperm granuloma (SG), adjacent to the “Clip Artifact” (long arrow) within the suprascrotal segment of the ductus (vas) deferens postvasectomy. |
 FIGURE 19-12 Scrotal ligaments. Longitudinal image of scrotal ligaments (SL, arrow) best seen in the presence of a hydrocele. Normal testis (T). |
 FIGURE 19-13 Tunica albuginea. Longitudinal image of testis demonstrating normal tunica albuginea (arrows). |
 FIGURE 19-14 Mediastinum testis. A: Longitudinal image of mediastinum testis (MT) seen as a bright, echogenic band of fibrofatty tissue across testis. B: Transverse image through mediastinum testis (MT) seen as a bright, echogenic area in testis at the 9-o’clock position. |
 FIGURE 19-15 Rete testis. Longitudinal image of normal testis showing echogenic stroma (arrow) with tubules of rete testis (RT). |
the cremasteric artery (a branch of the inferior epigastric artery).2,6,9,28 The deferential artery supplies the epididymis and vas deferens.2,6,7,9,11,28 Major blood supply to the epididymis, however, is via the superior epididymal artery, a branch of the testicular artery.6,11 The cremasteric artery supplies the peritesticular tissues (Fig. 19-18A, B). Both the deferential and cremasteric arteries also contribute a variable amount of blood to the testis via anastomoses with the testicular artery.2,7,9,28
 FIGURE 19-16 Appendix testis and appendix epididymis. A: Schematic illustration of appendix testis and appendix epididymis. B: Longitudinal image of testis (T) shows hydrocele and appendix testis (small arrows). Scrotal pearl is also seen (large arrows). C: Longitudinal image of normal testis (T) with appendix testis (arrow). Normal color flow is seen in the appendix. A small hydrocele is present. D: Longitudinal image of testis (T) with a cyst-like appendix epididymis (arrow) arising from the head of the epididymis (E). |
 FIGURE 19-17 Testis. A: On the longitudinal of the normal testis, the calipers were used to measure length (1) and the width (2). B: Transverse image of normal testis. |
 FIGURE 19-18 Vascular anatomy. Schematic illustration of normal arterial supply to the scrotum (A), intrascrotal arterial supply (B), and venous drainage form the scrotum (C). |
In approximately 50% of normal testes, a transmediastinal arterial branch of the testicular artery enters the mediastinum and courses through the testicular parenchyma in a direction opposite to that of the centripetal arteries to supply the capsular artery. A transmediastinal vein usually accompanies the artery.5,7,9, 10 and 11,28,29 The grayscale sonographic appearance of the transmediastinal artery is a prominent hypoechoic band traversing the testis5,9 (Fig. 19-19A). With color Doppler, the transmediastinal artery is seen as a prominent arterial branch traversing the mediastinum, demonstrating flow toward the periphery of the testis to supply the capsular arteries5,7,10,38 (Fig. 19-19B). Flow in the transmediastinal artery courses in the opposite direction relative to the centripetal arteries5,6,28
 FIGURE 19-19 Intrascrotal arteries. A: Transverse image of the testis showing the transmediastinal artery (TMA, arrow), entering the mediastinum testis (MT), traversing the testis to supply the capsular artery. B: Transverse color image of transmediastinal artery (TMA) entering the mediastinum testis (MT), supplying capsular artery (CA); (arrow) the transmediastinal vein (TMV) accompanies the artery, with color flow seen in the opposite direction (arrow). |
 FIGURE 19-20 Spectral and color Doppler images of intrascrotal arteries. A: Normal spectral waveform of an intratesticular artery demonstrating low-resistance flow. B: Normal spectral waveform of the epididymal artery with low-resistance flow. C: Normal spectral waveform of the spermatic cord with high-resistance flow from either the cremasteric or deferential arteries. D: Longitudinal oblique images demonstrating normal intratesticular arteries. Color Doppler shows blood flow away from the Mediastinum Testis (MT). The RR are the Recurrent Rami intratesticular arteries which are demonstrated with the arrows. The Mediastinum Testis is a network of fibrous connective tissue that supports the ducts and vessels as they pass into and out of the testicular parenchyma. |
TABLE 19-1 Sonographic Appearance of Common Scrotal Lesion | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
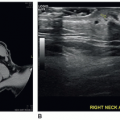
 FIGURE 19-21 Undescended testis. Longitudinal image of a small, undescended testis (arrows) located in the inguinal canal. MT, mediastinum testis. |
color or power Doppler to confirm the presence of arterial and venous flow within the testis because color Doppler can be subject to motion artifacts.13
 FIGURE 19-22 Testicular torsion. Longitudinal image of spermatic cord demonstrating “the knot” or “whirlpool” pattern (arrows) seen in testicular torsion. (Image courtesy of Dr. Vijayaraghavan S. Boopathy.) |
 FIGURE 19-23 Types of testicular torsion. A: Schematic illustration of intravaginal testicular torsion. B: Schematic illustration of extravaginal testicular torsion. |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


