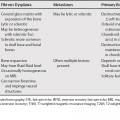
60 A solitary pulmonary nodule can be defined as a well- or poorly defined, roughly circumscribed, round or oval lesion measuring less than 3 cm in diameter. The only specific and reliable sign of the benign nature of a solitary lesion includes the identification of certain benign types of calcifications and the absolute absence of growth over a 2-year period. A solitary pulmonary nodule in a patient under the age of 35 years with no history of an extrathoracic malignancy is generally considered benign. Benign nodules generally have a doubling time (double in volume) of less than 1 month or more than 16 months. There is a significant overlap of growth rates among rapidly growing nodules (Table 60.1). Typically, malignant nodules enhance on contrast-enhanced chest computed tomography (CT). Active granulomas and other infectious lesions, however, can also show enhancement. Similarly, positron emission tomography (PET) imaging with glucose analog F18-fluorodeoxyglucose (FDG) shows increased glucose metabolism in metabolically active processes such as malignant nodules; however, inflammatory or infectious processes can also have increased FDG activity leading to a false-positive result (Table 60.2).
The Solitary Pulmonary Nodule
| Nodule Size (mm)b | Low-Risk Patientc | High-Risk Patientd |
|---|---|---|
| ≤4 | No follow-up needede | Follow-up CT at 12 mon if unchanged, no further follow-upf |
| >4 to 6 | Follow-up CT at 12 mon if unchanged, no further follow-upf | Initial follow-up CT at 6 to 12 mon then at 18 to 24 mon if no changef |
| >6 to 8 | Initial follow-up CT at 6 to 12 mon then at 18 to 24 mon if no change | Initial follow-up CT 3 to 6 mon, then at 9 to 12 and 24 mon if no change |
| >8 | Follow-up CT at around 3, 9, and 24 mon dynamic contrast-enhanced CT, PET, and/or biopsy |