Chapter 27 Thoracic Disc Access
In the thoracic spine, a single-needle technique is generally the technique of choice. However, the double-needle technique with either an 18 g with 22 g or 20 g with 25 g introducer and needle combination is acceptable. The thoracic disc is generally a smaller target than the lumbar disc, so a thinner diameter needle may allow for easier access. The needle tip can be modified as described in Chapter 2 to optimize needle navigation. It is currently acceptable to have the needle entry be contralateral to the more painful side, unless there are prohibiting issues. Multiplanar imaging will be used to best advance the needle into its final position.
Note: Please see page ii for a list of anatomical terms/abbreviations used in this book.
 Trajectory View (Figure 27–1)
Trajectory View (Figure 27–1)
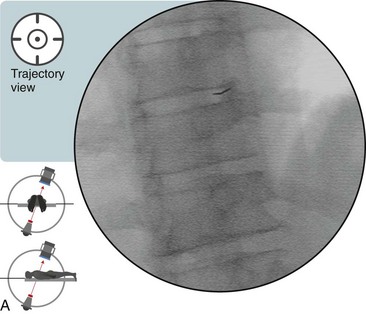
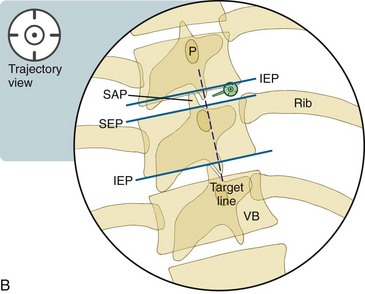
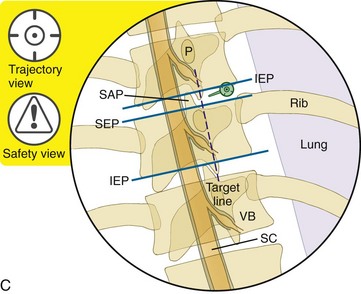
 Trajectory View Safety Considerations
Trajectory View Safety Considerations

 While advancing the needle toward the disc, do not go too far medial or lateral. Remain immediately lateral to the junction of the endplate and the SAP. Attempt to enter the disc “low in the hole” to avoid the exiting spinal nerve.
While advancing the needle toward the disc, do not go too far medial or lateral. Remain immediately lateral to the junction of the endplate and the SAP. Attempt to enter the disc “low in the hole” to avoid the exiting spinal nerve.
 Do not drive too far medial until entering the disc. A medial-straying needle can enter the dura.
Do not drive too far medial until entering the disc. A medial-straying needle can enter the dura.

 Notes on Positioning in the Trajectory View
Notes on Positioning in the Trajectory View
Related posts:
 Atlantoaxial Joint Intraarticular Injection
Atlantoaxial Joint Intraarticular Injection
 Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


