Chapter 12 Thoracic spine
The thoracic spine should not be routinely examined by radiography for pain without trauma, unless in the elderly when osteoporosis may cause sudden collapse of vertebrae. Magnetic resonance imaging (MRI) may be indicated if local pain continues.1
The clinical significance of wedge fractures should not be overlooked, as occasionally there may be fragments displaced within the spinal canal that could cause spinal cord compression.2
Indications
Fracture
The most common reason for examining this area radiographically is trauma, either major or minor, involving the region. Fractures of the upper and middle sections of the thoracic spine do not occur as frequently as those of the cervical vertebrae and thoracolumbar region. However, with thoracic spine fractures there is a higher incidence of spinal cord injury.3
Osteomyeloma
The thoracic spine may be examined as part of a skeletal survey to stage the condition and assess which lesions may benefit from radiotherapy.1
Anteroposterior (AP) thoracic spine (Fig. 12.1A, B)
Much research has been undertaken on the advantages and disadvantages of the posteroanterior (PA) versus the AP projection of the lumbar spine, particularly in relation to dose reduction. Brennan and Madigan,5 in their article analysing the PA projection of the lumbar spine, recommend the use of this procedure to facilitate dose reduction without loss of image quality. However, it must be remembered that, owing to the natural kyphotic curvature of the thoracic spine, oblique rays from the X-ray beam will be angled in the opposite direction to the intervertebral joint spaces. The resulting PA image is therefore not likely to demonstrate the intervertebral joint spaces as adequately as the AP projection. This is somewhat unfortunate, as the PA projection may reduce radiation dose to the breast, eyes and thyroid, all radiosensitive areas. However, breast shields may be used, and with good collimation this can significantly reduce the dose. Levy et al. have studied the use of the PA projection in examining the whole spine for scoliosis in adolescents.6 Their work suggests that a PA study of the spine will effect a reduction in dose to the patient without any loss of image quality, and although the assessment for scoliosis using plain radiography has reduced significantly with the increased use of other imaging methods, their work indicates that PA thoracic spine examination may be a possibility in some cases.

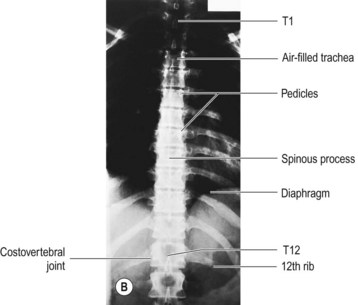
Figure 12.1 AP thoracic spine.
(B) Reproduced with permission from Bryan GJ. Skeletal anatomy. 3rd ed. Edinburgh: Churchill Livingstone; 1996 and Gunn C. Bones and joints. 4th ed. Edinburgh: Churchill Livingstone, 2002.
1 A high enough kVp can be used to reduce the subject contrast along the length of the spine.
2 A wedge filter can be used with the thicker end at the upper region of the thoracic spine.
3 A flour filter can be used, consisting of flour inside a radiolucent bag (usually plastic, which is covered by a cotton bag that can be washed). The contents of the bag can be shaken to distribute the flour into a thicker layer at one end; this thicker end of the bag is then placed over the upper end of the sternum and the flour is patted by the radiographer until the thickness decreases towards the lower end of the thoracic vertebrae. The filter is therefore adaptable to any patient size, unlike set-size aluminium filters. The filter can be made extremely cheaply and requires no specialist attachment feature on the light beam mounting, although manufacture of such a filter should only be attempted after consultation with health and safety and cross-infection specialists from the hospital where the filter is to be used.
Some texts suggest the use of the anode heel effect to help reduce the subject contrast along the length of the spine.7,8 However, it must be suggested that this is a somewhat outdated approach: anode targets in modern X-ray tubes are set at such an angle that this effect will have little or no difference on the resultant image.
The AP thoracic spine is exposed on arrested inspiration to ensure the diaphragm is lowered and a maximum number of thoracic vertebrae are demonstrated. However, it has also been suggested that the use of arrested expiration to reduce the amount of air in the thorax will provide a more uniform density over the thoracic spine, by helping to reduce the subject contrast of the air-filled lungs against the mediastinum and spine.8,9 This is a questionable suggestion in that there will always be air in the lung fields, even in expiration.
IR is horizontal, employed with antiscatter grid.
Positioning
• The patient is supine with their arms at their sides and legs extended
• A low radiolucent pillow or pad may be used to support the head, and the knees may be supported slightly with a pad for comfort
• A lead rubber apron is applied to the lower abdomen for gonad protection
• The median sagittal plane (MSP) is at 90° to the table-top and the coronal plane is parallel to the table-top



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


