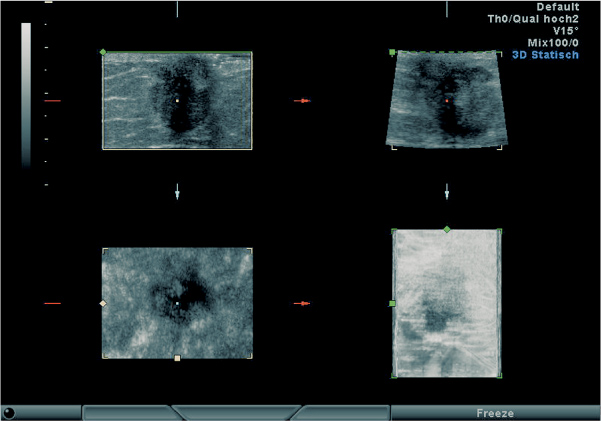
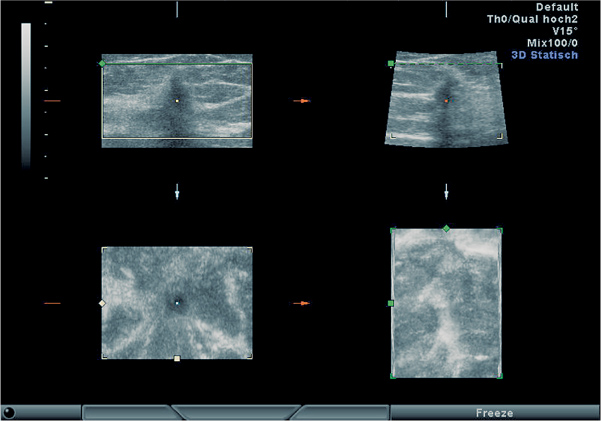
18 Three-dimensional, Extended Field-of-View Ultrasound, and Real-time Compound Scanning 3D ultrasound imaging has attained a high level of quality, but its dependence on the examiner continues to be a problem. The ability to visualize structures in three dimensions plays a major role in this regard. The ability to form a three-dimensional mental picture varies greatly among different examiners, and it can be learned only to a degree. Examiners who are poor visualizers will have great difficulties in conducting examinations and interpreting the findings. This leads to yet another problem: documentation and reporting the findings to another physician. Even if the sonographer has acquired a good three-dimensional impression of the disease process, it is still difficult to share that impression with another physician. This problem is particularly acute in cases where the recipient of the ultrasound report will also carry out the breast surgery. As a rule, the ultrasound documentation consists of two-dimensional images that show a lesion in cross section but do not convey a spatial impression of the lesion or its location in the tissue. This also makes it difficult to compare ultrasound findings with the results of other studies such as mammography or MRI. A common makeshift solution is to make line drawings of the lesion and describe its location as accurately as possible. But because malignant tumors are not simple geometric figures, it is very difficult to document and describe their shape and extent, especially if the lesions are multifocal. Given the complexity of breast anatomy, then, a reasonable approach is to represent the lesion and the surrounding organ in three dimensions. This can be accomplished by acquiring and storing three-dimensional image data and rendering the images in an extended or three-dimensional format. This also permits other examiners to repeat the breast examination and review suspicious findings even when the patient herself is no longer available. Another problem of ultrasound is that the small field of view under the transducer demonstrates only a small section of the whole breast. A sectional image of the lesion without the surrounding tissue makes planning for surgery and also comparison with mammography and MRI difficult. A panoramic scan enables the investigator to produce a two-dimensional cross-sectional image of the whole breast. In comparison with the small field of view under the real-time transducer, this allows much better recognition of the whole breast anatomy and the localization of a lesion within the breast. In conventional ultrasound sound is always transmitted in one direction only, producing a simple scan image. One of the important physical limitations of ultrasound is that good reflection of sound is only given if the ultrasonic beam hits structures in a perpendicular angle. If the angle of sound inclination is oblique, refraction occurs and the structure cannot be displayed. Breast anatomy is rather complex with many reflectors in variable directions. Therefore conventional ultrasound is limited with regard to demonstrating all breast structures. Compared with simple scanning, a compound image is created by image reconstruction from multiple scan directions. This improves the display of architectural details considerably. The principle of three-dimensional ultrasound is based on the acquisition and storage of numerous two-dimensional images in contiguous or closely spaced planes of section. Generally this requires a direct mechanical linkage and an automated method of moving the transducer through the various image planes so that the planes can be accurately localized. Systems have been designed for accomplishing this electronically, but this requires a very smooth, steady movement of the transducer combined with a time-triggered relay that stores the sectional planes at equally spaced intervals. The stored image data can be processed and displayed in various ways. Perhaps the most realistic display mode would be a transparent image in which the tumor could be viewed in three dimensions through the normal breast anatomy. In fetal examinations, for example, such a transparent display is excellent owing to the high contrast between the tissue (fetus) and the surrounding amniotic fluid, but because of the large number of similar gray levels that coexist within the breast it poses serious technical difficulties at present. High contrast is also desirable for constructing three-dimensional surface-rendered images. But this degree of contrast is unusual within the breast, and so for the time being other means are needed for representing structures in three dimensions. The simplest method is to image a representative sectional plane and then reconstruct the two planes that are perpendicular to the original plane to create an orthogonal multi-planar display (Figs. 18.1–18.6). If these planes were reconstructed along fixed, predefined spatial axes, they could not depict the complex geometry that is typical of malignant tumors. However, complex growth patterns can be appreciated if the image planes can be freely rotated in space. At present, three-dimensional structures in breast ultrasound are most clearly represented by a volume block in which a sectional slice from the tumor can be interactively displayed in arbitrary spatial planes (Figs. 18.1–18.7). Fig. 18.1 Invasive ductal carcinoma, size 12 × 17 × 14 mm. Sectional planes reconstructed from the volume acquisition: sagittal (upper left), transverse (upper right), horizontal (C scan, lower left), and transparent display (lower right). The slice thickness for the transparent mode has been selected to large. Therefore the tumor is partly covered from the surrounding breast tissue. The C scanning plane clearly shows the typical retraction pattern of carcinomas. Fig. 18.2 Early invasive ductal carcinoma, size 5 × 6 × 5 mm. The horizontal C plane at lower left clearly shows the retraction sign. The lower right image displays the transparent mode. As in Fig. 18.1 the slice thickness has been selected to large and therefore the tumor is completely hidden through the surrounding fibroglandular tissue. Another method of image reconstruction involves extending the image plane itself. A basic limitation of ultrasound is the small field of view, especially with high-resolution transducers, which usually have an image field width of 4 cm or less. The old water-bath immersion scanners had a great advantage in this regard, as they could provide two-dimensional survey images of the entire breast. Today, real-time scanners are used almost exclusively because of their better spatial resolution, but the small field of view taxes the examiner’s ability to visualize the breast anatomy (see also Chapter 2
Clinical Significance
Extended Field-of-View Ultrasound
Real-time Compound Scanning
Technical Principles – 3D
Extended Field-of-View-Ultrasound
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


