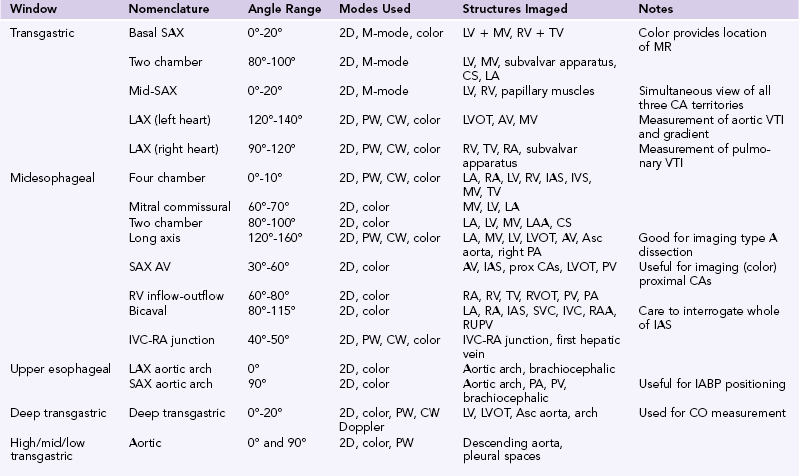
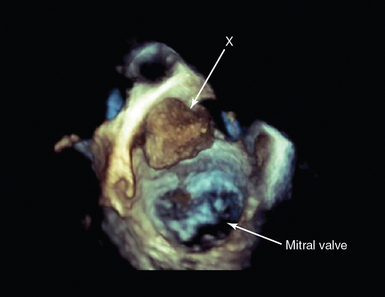
29 After development of an esophageal stethoscope, the first transesophageal echocardiographic (TEE) equipment provided simple M-mode images to measure left ventricular (LV) dimensions. First used for intraoperative monitoring of LV function and intracardiac air more than 30 years ago,1 TEE is now widely considered the standard of care for a number of cardiac surgical procedures.2,3 In parallel with transthoracic echocardiography (TTE), development of phased-array transducers; spectral and color Doppler; biplane, multiplane, and three-dimensional (3D) imaging; and progressive miniaturization of equipment has increased the quality and range of information available from the technique. For 20 years it has been recognized that TEE can provide additional information to other hemodynamic monitors (including the pulmonary artery catheter), which changes patient management and may improve outcomes.4 Currently, in the United States, the majority of anesthesiologists trained in TEE believe the technique to be superior to other hemodynamic monitors.5 Guidelines for performance of and training in TEE have been published by a number of national and international bodies (see Chapter 27). Although in general, TTE should be the first imaging mode used, its usefulness in the intensive care unit (ICU) may be limited by the patient (immobility, body habitus, pulmonary pathology), the pathology (i.e., prosthetic valve endocarditis), or ICU interventions (intermittent positive-pressure ventilation [IPPV], dressings/drains). In these instances, TEE may be required. Despite not being considered essential for basic critical care echocardiography, TEE is increasingly regarded as an essential skill for those who wish to perform more advanced ICU echocardiography,6,7 with experienced practitioners using the two techniques in a complementary and potentially interchangeable manner. This comprises a miniaturized ultrasound transducer incorporated into a custom-made transesophageal probe. The device uses an array of piezoelectric crystals and phased-array technology to steer the ultrasound beam through 180 degrees. The frequency range used varies (generally) between 5 to 10 MHz, and all modalities available in TTE are potentially available for TEE, including the ability to acquire real-time high-quality 3D images (Figure 29-1). Progressive technologic development has allowed availability of pediatric and neonatal TEE probes, and a disposable miniaturized probe has been devised for use as a continuous hemodynamic monitor in the ICU. Figure 29-1 Three-dimensional (3D) transesophageal echocardiography (TEE). 3D-TEE in a patient presenting with acute cerebrovascular accident in multiple carotid artery territories. The image is a full-volume rendition, manipulated to be looking down on the mitral valve from the roof of the left atrium. There is a mass (X) attached to the atrial wall. At surgery, this was shown to be a left atrial myxoma. This should include infection control (knowledge of local and national guidelines, probe sterilization, cleaning, and tracking), and care of the probe (including procedures for checking integrity before each use). Nasogastric tubes are often in situ, and to ensure interruption of feed is minimized, gastric contents should be aspirated before the study, and postprobe removal protocols should be in place to ensure no displacement has occurred, and feeding is recommenced only and as soon as judged safe.3,7 The process of consent varies between countries, and although invasive procedures are usually undertaken only after consent is obtained, exceptions are generally allowed in the case of life-threatening emergencies and/or when the patient is unable to give informed consent. In some countries, informing the patient’s documented next of kin before a nonemergency invasive procedure is normal practice. Where research is undertaken, ethical approval must be obtained and consent obtained according to the agreed research protocol and local guidelines. The study should be recorded and reported according to local, national, and international guidelines and recommendations. This should include the indication for TEE and the patient history in terms of the relative and absolute contraindications to TEE (Table 29-1) and to its risk-benefit to the patient. The most significant serious complication from TEE in the outpatient population is esophageal perforation, with the usually quoted rate of 1:10,000 in studies; however, this is variable and may increase with an increasingly aged patient population.8 TEE in the intensive care is generally regarded as safe; however, because the critically ill patient is frequently coagulopathic, knowledge of the coagulation status of the patient is vital and, where indicated, possible correction undertaken. When the patient is fully anticoagulated or coagulopathic, probe insertion with laryngoscopic guidance is recommended. This is important if the patient is receiving extracorporeal support; in this circumstance, oropharyngeal bleeding can be life threatening. Critically ill patients undergoing TEE will be intubated and ventilated, and consistent with guidelines in many ICUs, there should be an independent ICU practitioner managing the airway, ventilation, and hemodynamic status of the patient during the study. TABLE 29-1 Contraindications to Transesophageal Echocardiography3,7,8 Guidelines for performance of a comprehensive TEE study have been published, with recommendations for a minimum dataset in a number of circumstances.3,7 The practitioner will then focus on the specific question that requires answering. In existing guidelines and recommendations, these predominantly relate to the perioperative cardiac surgical setting; however, it is not the mode of echo (TTE vs. TEE) but, rather, the information required that drives the study. Indeed, in undertaking repeated focused studies and/or using TEE as a hemodynamic monitor, only limited views may be required. The standard order of image acquisition depends upon a number of factors, including the urgency of the study and time frame for acquisition, the type (comprehensive vs. focused), and individual practitioner preference. Ideally, in the critically ill patient, the amount of probe manipulation should be minimized, in particular in the elderly and/or coagulopathic patient. Movement of the probe is described in terms of its position with respect to the patient: withdraw/advance, rotate left/right, anteflex/retroflex, and flex right/left. Additional movement of the ultrasound beam relates to electronic rotation (from 0-180 degrees). As with TTE, as there is anatomic variation between patients, although numbers are given regarding the degree of electronic rotation, these are for guidance only. The standard views are described in Table 29-1, together with the main structures seen (Table 29-2). Of note, the deep transgastric view is not achievable in all patients. Again, care should be taken to avoid excessive probe manipulation. Imaging of the pulmonary veins can be achieved by standard views (as described in Table 29-1) and additionally at 0 degrees, interrogating the right and left sides of the left atrium (both superiorly and inferiorly) in turn. The indications for echocardiography in the ICU have been discussed in Chapters 26 and 27, including the choice of TTE versus TEE. Images of diagnostic quality are unobtainable in up to 30% of the general ICU patient population, rising to 85% in those with severe, acute respiratory failure referred for extracorporeal respiratory support (Figure 29-2).9 Thus, when image quality precludes obtaining adequate information from the transthoracic route, TEE may be indicated. In addition, there are specific indications for TEE as opposed to TTE (Table 29-3). Guidelines for the appropriateness of undertaking TEE have been published; however, these will inevitably change with the ongoing development of critical care technologies, for example, extracorporeal support.10,11 TABLE 29-3 Specific Indications for Transesophageal Echocardiography
Transesophageal echocardiography
Overview
The TEE probe
Preparation for TEE in the critically ill
Process review
Patient review
Relative
Absolute
History of esophageal surgery
Esophageal obstruction
Esophageal varices or diverticulum
Esophageal stricture
Gastric/esophageal bleeding
Poor airway control
Oropharyngeal pathology (i.e., pharyngeal pouch)
Severe coagulopathy
Cervical spine injury
Image acquisition: The standard views
Indications for transesophageal echocardiography in the critically ill
Indication
Notes
Intracardiac thrombus/mass
Most commonly, LAA thrombus in patient with AF
May see LV thrombus related to akinetic segment (NB apex difficult to visualize with TEE)
Potential for paradoxic embolization with PFO/ASD
Endocarditis
Prosthetic valve endocarditis frequently paraprosthetic leak only
Infection may be associated with indwelling lines/wires
All patients, expert echocardiographic review required
Extracorporeal support
Useful for insertion and positioning of IABP
ECMO and VAD: Highly specialized echocardiography
Aortic disease
Not all the aorta can be imaged, alternative imaging may be required
Aortic dissection: Origin of coronary arteries (true vs. false lumen)
Valvular disease
Mitral
MR may be dynamic, stress +/− volume loading may be required
Assess mechanism of MR
Critical MS: Suitability for valvuloplasty
Indicated to assess potential prosthesis malfunction
Aortic
Critical AS: Suitability for valvuloplasty
Indicated to assess potential prosthesis malfunction
Cardiac monitoring
Multiple potential uses; however, operator dependent and intermittent measure of cardiac function
Unexplained hypoxia
Intracardiac shunting not uncommon in ventilated patients
Potential to visualize intracardiac/pulmonary artery thrombus
Tamponade
Related posts:
 Ultrasound-guided peripheral intravenous access
Ultrasound-guided peripheral intravenous access
 Ultrasound-guided arterial catheterization
Ultrasound-guided arterial catheterization
 Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
 Use of ultrasound in the evaluation and treatment of intraabdominal hypertension and abdominal compartment syndrome
Use of ultrasound in the evaluation and treatment of intraabdominal hypertension and abdominal compartment syndrome
 Ultrasound imaging in space flight
Ultrasound imaging in space flight
 Approach to the urogenital system
Approach to the urogenital system
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access