Traumatic Facial Injury
Aimee Lynn Maceda
Monica D. Watkins
Radiologic consultation for facial trauma is common in the emergency room setting. Most facial fractures occur secondary to direct blow to the face with the remainder mainly due to automobile accidents. Nasal fractures are the most common, followed by mandibular and zygomatic fractures. High speed automobile accidents commonly result in zygomaticomaxillary and LeFort midfacial fractures.
Adequate evaluation of facial fractures requires thin slice computed tomography (CT) with multiplanar reconstructions. The probability of facial fracture is extremely low if there is no nasal bone fracture and fluid in the paranasal sinuses.
Unilateral facial fractures most commonly represent zygomaticomaxillary complex (ZMC) fracture. Orbital fracture account for most other unilateral fractures (discussed in Chap. 4, “Orbital Fractures”).
Nearly all bilateral facial fractures represent Le-Fort fractures.
All LeFort fractures involve pterygoid processes.
Each LeFort fracture has a unique component.
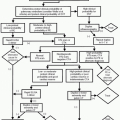
LeFort I: “Floating Palate” (Fig. 3-1)
Frequency: 20-30% of LeFort fractures.
Examination: maxillary teeth moveable on physical examination.
Mechanism: directed horizontal impact to the premaxilla.
Unique component: inferior orbital rim.
All components: horizontal fracture through inferior nasal septum, floor of the maxillary sinuses (anterior, medial, lateral, and posterior walls), and bilateral pterygoid plates.
LeFort II: “Floating Maxilla, Pyramidal Fracture” (Fig. 3-1)
Frequency: 35-55% of LeFort-type maxillary fractures; the most common type.
Examination: the midportion of the face is detached resulting in movement of the maxillary teeth and nose relative to the remainder of the skull.
Mechanism: horizontal blow to the midportion of the face.
Unique component: inferior orbital rim.
All components: pyramidal-shaped fracture with the nasofrontal suture at the apex and the teeth as the base. Fracture passes through the nasal ala across the frontal process of the maxilla and medial orbital wall. The fracture then extends through the infraorbital rim and then involves the posterior and lateral wall of the maxillary sinus. The fracture line then crosses the pterygomaxillary fossa and through the pterygoid plates.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree