Presentation and Presenting Images
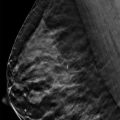
( ▶ Fig. 10.1, ▶ Fig. 10.2, ▶ Fig. 10.3, ▶ Fig. 10.4)
A 73-year-old female with a history of left breast cancer treated with lumpectomy and radiation therapy more than 10 years ago presents for screening mammography.
10.2 Key Images
10.2.1 Breast Tissue Density
There are scattered areas of fibroglandular density.
10.2.2 Imaging Findings
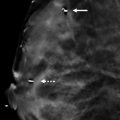
In the upper outer quadrant of the left breast in the middle depth at the 2 o’clock location, there is architectural distortion ( ▶ Fig. 10.5 and ▶ Fig. 10.6). It is located inferior and posterior to the radiopaque line marker placed on the skin over the surgical scar.
10.3 BI-RADS Classification and Action
Category 2: Benign
10.4 Differential Diagnosis
Lumpectomy surgical scar: Scars from surgery can have a variable appearance from person to person and within a person over time. The proximity of the architectural distortion to the skin marker and also the clinical history strongly favor that that this architectural distortion is due to surgery.
Recurrent cancer: The changes are stable from prior mammograms (not shown). There does not appear to be a new mass, increased density, or calcifications, which would suggest recurrence.
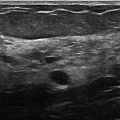
Skin-fold changes: The changes appear to be internal to the breast. Skin folds and skin lesions can simulate breast lesions; however, the digital breast tomosynthesis (DBT) images would localize the findings to the skin.
10.5 Essential Facts
Skin markers on surgical scars can greatly assist in determining if an architectural distortion is due to surgery or represents a finding needing further evaluation.
Similar to conventional mammography, postsurgical changes seen on DBT should have similar appearances and conventions (and intervals) for following to ascertain stability and change.
Typical breast-conserving–treatment (BCT) changes are skin thickening, increased parenchymal markings, a stellate or masslike density at the surgical site, and dystrophic calcifications. These changes will vary over time.
The lumpectomy site appears as a spiculated, poorly defined soft-tissue density with interspersed radiolucent areas of trapped fat.
10.6 Management and Digital Breast Tomosynthesis Principles
Architectural distortion seen on DBT that is not attributed to a surgical scar and not seen on mammography or sonography should be considered suspicious. Biopsy would be warranted. DBT needle localization or DBT-guided core needle biopsy are options for tissue sampling.
Patients treated with BCT have a long-term risk of recurrence estimated at 1 to 2.5% per year.
Recurrence at a lumpectomy site is suggested by the lack of central radiolucent areas, a central mass, fine straight spiculations, and an increase in size or nodularity of the scar. On DBT, a partial central lucent area may be seen due to the unmasking of the summation effects of conventional mammography.
10.7 Further Reading
[1] Dershaw DD. Breast imaging and the conservative treatment of breast cancer. Radiol Clin North Am. 2002; 40(3): 501‐516 PubMed
[2] Freer PE, Niell B, Rafferty EA. Preoperative Tomosynthesis-guided Needle Localization of Mammographically and Sonographically Occult Breast Lesions. Radiology. 2015; 275(2): 377‐383 PubMed
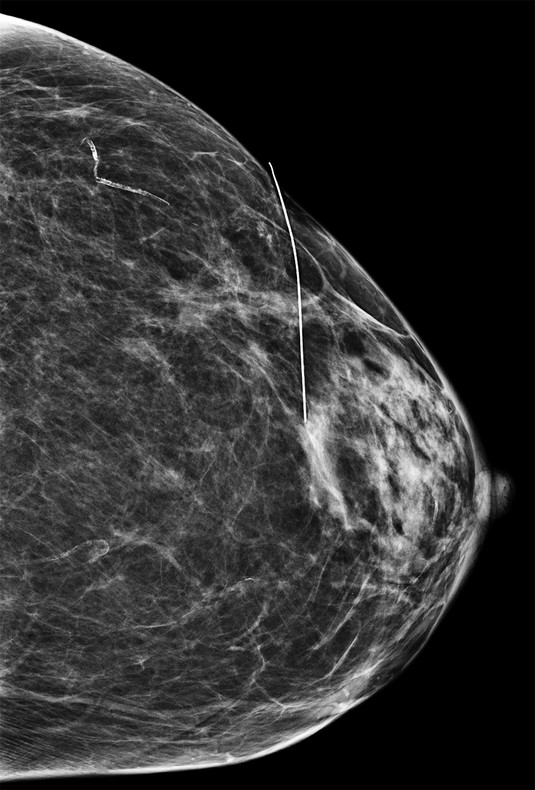
Fig. 10.1 Left craniocaudal (LCC) mammogram.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


