CHAPTER 14 Tumors of the small and large intestine









Introduction
Small and large intestinal tumors are broadly classified into non-neoplastic (or tumor-like lesions) and neoplastic tumors (Table 14.1) most of which are epithelial (arise from the surface epithelium) and the minority are non-epithelial tumors (stromal). Non-neoplastic lesions are those which follow a benign course and do not have a tendency for malignant transformation as opposed to neoplastic tumors, which are pre-malignant from which carcinoma arises (Kumar et al., 2004; Robertson and Levison, 2006).
Table 14.1 Classification of tumors of small and large intestines
Colorectal cancer is a major cause of morbidity and mortality worldwide (Geboes et al., 2005). Around 100 new cases of colorectal cancer are diagnosed each day in the UK and it is the third most common cancer after breast and lung (Cancer Research UK, 2007). Epithelial tumors of the small intestine are rare compared to the large intestine.
Both neoplastic and non-neoplastic lesions of the small and large intestines commonly present in the form of a polyp, which is defined as a raised lesion above the mucosa that protrudes into the lumen of the digestive tract (Geboes et al., 2005).
Non-neoplastic/tumor-like lesions
Hyperplastic/metaplastic polyps and serrated adenomas
Hyperplastic polyps are benign epithelial lesions that are usually small and less than 5 mm in maximum diameter. By definition, they do not display dysplasia (see glossary for definition) and, in most instances, they are not pre-neoplastic in nature. They are usually asymptomatic and can be multiple and they mainly involve the large intestine rather than the small intestine (Robertson and Levison, 2006). Histologically, they are composed of well-formed glands lined by non-neoplastic epithelial cells, most of which show maturation with small, regular nuclei located in the base of the cells (Geboes et al., 2005). They are found in approximately 40% of rectal specimens in people younger than 40 years and in 75% of older persons (Rubin and Strayer, 2007). They are usually limited to the large bowel and are believed to arise due to a defect in proliferation and maturation of normal mucosal epithelium (Geboes et al., 2005). Typically, the luminal epithelium shows hyperplastic change with the typical intraluminal infoldings resulting in a saw-toothed appearance (Rosai, 2004; Geboes et al., 2005). By definition, hyperplastic polyps have no malignant potential; however, this stance has recently been challenged and, in some cases, adenocarcinomas of the colon have been found to contain residual adenomatous and hyperplastic epithelium (Robertson and Levison, 2006). In patients with hyperplastic polyposis syndrome, the polyps tend to be large and sometimes associated with adenocarcinoma (Leggett et al., 2001). Recently, on the genetic level, these polyps are shown to contain K-ras mutation which is a mutation commonly associated with colorectal cancer (CRC) (Day et al., 2003).
In recent years, there has been growing evidence that there is a subgroup of hyperplastic polyps that are not homogeneous and are termed serrated adenomas. They are polyps showing both hyperplastic and adenomatous change (Longacre and Fenoglio-Preiser, 1990) and have a higher incidence of microsatellite instability (see glossary for definition) and increased risk of development of carcinoma (Day et al., 2003).
Hyperplastic polyposis encompasses a large number of hyperplastic polyps, which are distributed throughout the large bowel and are usually more than 1 cm in size (Williams et al., 1980). This disease is associated with increased risk of malignancy and usually associated with adenomatous polyps.
Juvenile polyps
These represent focal hamartomatous non-neoplastic malformations of the mucosal epithelium and the vast majority occur in children less than 5 years of age (Robertson and Levison, 2006). Most involve the rectum with an equal male and female distribution and gastrointestinal bleeding is the most common presentation (Day et al., 2003).
Histologically, the lamina propria is usually abundant and encloses cystically dilated glands together with abundant inflammation and frequent ulceration. They have no malignant potential (Nugent et al., 1993). However, when they occur in the setting of juvenile polyposis syndrome (a rare autosomal dominant disease), they do carry a higher risk of malignancy and, in this setting, most cancers occur between the age of 20 and 40 years (Robertson and Levison, 2006).
Peutz-Jeghers (PJ) polyps
These are also a hamartomatous type of lesion that involve the upper and lower gastrointestinal tract and are more frequently found in the small bowel rather than the large bowel. They usually occur in the setting of Peutz-Jeghers (PJ) syndrome, which is an autosomal dominant hereditary condition that is associated with mucosal and cutaneous pigmentation around the lips, oral mucosa, face and other parts of the body (Haggitt and Reid, 1986). Histologically, they are composed of arborizing connective tissue with well-developed smooth muscle fibers that extend into the surrounding mucosa and the lamina propria to surround the crypts (Fulcheri et al., 1991). Patients with PJ polyps commonly present with gastrointestinal hemorrhage and anemia, recurrent colicky abdominal pain and sometimes with recurring intussusceptions, especially after a meal in younger patients (Day et al., 2003). Patients with PJ syndrome have a higher risk of developing gastrointestinal and non-gastrointestinal tumors such as breast and ovarian malignancies (Trau et al., 1982).
Inflammatory polyps
These benign polyps can complicate any inflammatory/infectious disease of the gastrointestinal tract and commonly occur in the setting of inflammatory bowel disease (ulcerative colitis and Crohn’s disease), mucosal ulceration and in the mucosal prolapse syndrome. They can complicate certain infectious conditions of the bowel, for example schistosomiasis and amebiasis (Robertson and Levison, 2006). They are usually multiple and occur as a non-neoplastic proliferation of either mucosa or granulation tissue due to various injuries to colorectal epithelium. Histologically, they are composed of a pedunculated mucosal growth that is composed of inflammation and commonly associated with surface ulceration and granulation tissue formation. They are benign polyps and have no propensity for malignant transformation (Robertson and Levison, 2006).
Benign neoplastic epithelial tumors
Adenomatous polyps
Adenomas are benign neoplastic polyps derived from the surface epithelium and occur in both small and large intestines, involving the latter more frequently (Perzin and Bridge, 1981). Adenomas, by definition, are pre-malignant lesions with increased risk of malignant transformation (Leslie et al., 2002). In the small bowel, most benign adenomas occur in the region of the ampulla of Vater and generally they occur most frequently in the region of the duodenum and jejunum and less frequently in the ileum (Rubin and Isaacson, 1990; Cooperman et al., 1978).
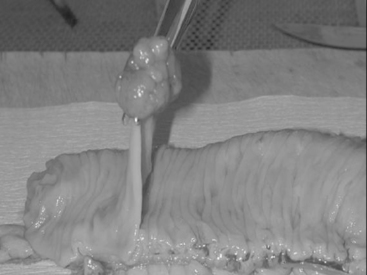
Macroscopically, adenomas can be classified as either sessile or pedunculated. Sessile polyps are attached to the mucosa without a stalk and are usually raised, while peduculated polyps have a stalk (usually composed of normal mucosa) of variable length attached by a narrow base (Figures 14.1 and 14.2) (Robertson and Levison, 2006; Rubin and Strayer, 2007).





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


