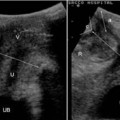
Fig. 3.1
Proximal portion of the anal canal at transanal ultrasound. a Anal canal at the level of the anorectal junction as recognized by the puborectalis sling, which creates a hyperechoic U-shaped formation around the posterior wall of the anal canal. b Middle portion of the canal. The puboec- talis muscle blends with the external sphincter, creating a complete ring
the anorectal junction to 1 cm below the dentate line and is composed of smooth muscle fibers. The internal anal sphincter is seen as a hypoechoic symmetric ring (Fig. 3.2) and is best visualized in the middle part of the anal canal, where it is thickest and uniformly hypoechoic. It is sharply demarcated from the heterogeneous subepithelial tissues medially and the longitudinal muscle laterally.
The circular-shaped external anal sphincter is the outermost muscle of the distal anal canal. While shorter anteriorly in women, it extends approximately 1 cm beyond the internal anal sphincter (Fig. 3.3). The deep part of the external anal sphincter is fused with or intimately related to the puborectalis muscle. Anteriorly, it is closely related to the superficial transverse muscle of the perineum and perineal body, which is seen as a hypoechoic anterior region on transanal ultrasound. The external anal sphincter shows a fibrillar pattern of fine parallel hyperechoic lines in the proximal third of the anal canal (deeper part of the external anal sphincter) which become more homogeneous in the distal third (superficial or subcutaneous part of the external anal sphincter). Although the external sphincter and longitudinal muscle are relatively heterogeneous, they can be distinguished by performing the examination with 10MHz transducers. Between the two cylindrical layers of the sphincters is the
intersphincteric space, which is visible on transanal sonography as a hypere- choic band sometimes together with a hypoechoic longitudinal muscle, the latter being the continuation of the rectal wall (Fig. 3.4). Therefore, the intersphincteric space may show mixed echogenicity.
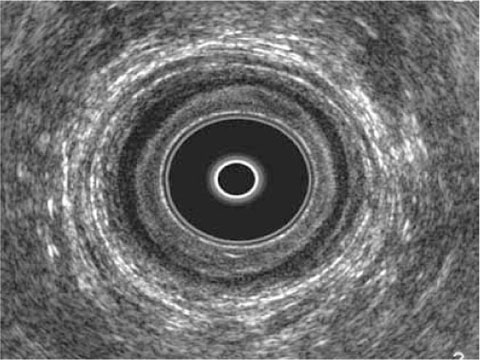
Fig. 3.2
Internal anal sphincter at transanal ultrasound. Tranverse section of the internal anal sphincter, observed as thick hypoechoic symmetric ring in the middle of the anal canal. It is sharply demarcated from heterogeneous subepithelial tissues medially and the longitudinal muscle laterally
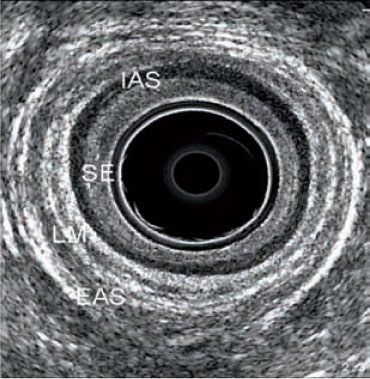
Fig. 3.3
External anal sphincter at transanal ultrasound. Transverse section of the external anal sphincter observed as a circular structure with a typical fibrillar pattern whose deep parts are fused with the puborectalis muscle. IAS internal anal sphincter, SE subepithelial tissue, LM longitudinal muscle, EAS external anal sphincter
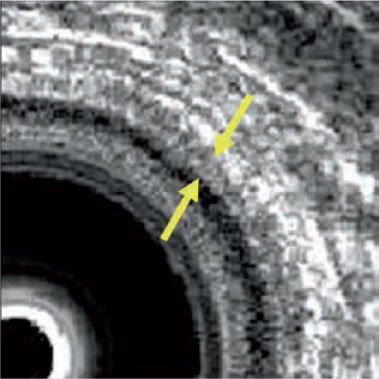
Fig. 3.4
Intersphincteric space at trans-anal ultrasound. It is visible as an hyperechoic band inside the hypoechoic longitudinal muscle (arrows)
Measurements of muscle thickness are clinically important because they are central to the diagnosis of sphincter atrophy and the assessment of fecal incontinence. Transanal ultrasound enables reliable measurement only of internal sphincter thickness, whereas with MRI, especially endoanal MRI, all sphincter components can be reliably measured [3




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
