Ultrasound pattern
Estimated risk of malignancy (%)
FNA size threshold
High suspicion
>70–90
≥1 cm (repeat FNA within 12 months if initial cytology is benign)
Intermediate suspicion
10–20
≥1 cm
Low suspicion
5–10
≥1.5 cm
Very low suspicion
<3
≥2 cm or consider observation
Benign
<1
No biopsy
Table 12.2
AACE/ACE/AME 2016 guidelines for UGFNA of thyroid nodules
Ultrasound pattern | Estimated risk of malignancy (%) | FNA size threshold |
|---|---|---|
High risk | 50–90 | ≥1 cm |
Intermediate risk | 5–15 | ≥2 cm |
Low risk | <1 | ≥2 cm or growing |
The question of whether to biopsy nodules less than 1 cm (micronodules) remains controversial. These micronodules have the same risk of malignancy as larger nodules with similar sonographic pattern [8, 9] but seldom present a threat. Small nodules are common in the population, and routine biopsy of all potentially suspicious micronodules is not likely cost-effective or clinically beneficial. Clearly some judgment is required in deciding which nodules require FNA. Careful ultrasound evaluation can identify suspicious lymph nodes and high-risk micronodules located at the thyroid capsule with potential invasion into the recurrent laryngeal nerve, trachea, or strap muscles, findings which may prompt FNA over surveillance. These features, when combined with patient age and comorbidities, can aid in clinical decision making [10, 11].
Preparation for UGFNA
Prior to consideration of a thyroid nodule aspiration, a history of relative contraindications and rarely absolute contraindication should be obtained. These include patients who may not be able to lie recumbent due to physical problems, who have difficulty in controlling the rate and depth of respiration, and who are uncooperative because of anxiety. Instead of the recumbent position , UGFNA may be performed at 45–60° elevation of the upper body or in a semi-sitting position. Patients with breathing issues or anxiety may often do well with discussion, reassurance, and directions given during the procedure. Nodule FNA tends to be less painful than lymph nodes (due to overlying sternocleidomastoid muscle), and pain generally correlates with anxiety, young age, and the number of nodules biopsied [12, 13]. Younger children may require anesthesia or sedation, while adults can be premedicated with an anxiolytic medication in order to obtain a satisfactory biopsy provided someone is able to drive them to and from the procedure.
A written and signed informed consent should be obtained after a verbal discussion during which all questions have been answered. Latex or anesthetic allergies should be documented. The consent form should contain in lay language all details and additional information regarding the reason for the procedure who will be performing the UGFNA, a description of the procedure and risks, the possibilities of false-negative results and not obtaining an adequate sample, and patient and witness signatures.
Thorough discussion prior to the procedure usually minimizes patient anxiety. This explanation should include that patients will feel a strange pressure briefly (as the needle passes through strap muscles), and sometimes pain radiates to the ear, jaw, or upper chest. Patients should not hold their breath during the procedure and should be told not to talk or move. Advising patients not to swallow may increase the chance of swallowing during the FNA. Patients should be told of potential complications [14]. Vasovagal reactions are self-limited and managed by keeping patient supine with legs elevated and a cold compress to forehead. After instructions should include possibility of bruising, recommendations for ice/acetaminophen if pain/swelling (nonsteroidal anti-inflammatory agent after 48 h if needed), and clear communication on how results will be conveyed to the patient.
Fine Needle vs. Core Biopsy
An UGFNA biopsy is defined as utilizing a 25 or 27 gauge needle. Larger needles, cutting needles, coring needles, and spring-loaded, needle projecting devices all have an inherently greater risk for significant bleeding. Also, there is greater risk for puncture site infection and for structural damage to the thyroid, trachea, esophagus, carotid artery, jugular vein, and recurrent laryngeal nerve [15]. Larger needles do not aid in further defining cytologically benign from malignant (indeterminate) follicular nodules but may have a role when FNA shows atypical cytology [16]. Core needle biopsy can help in obtaining an adequate sample for cytologic interpretation after two or three repeated FNA “nondiagnostic” aspirates [17]. Thus, the use of an ultrasound-guided, 25 or 27 gauge FNA biopsy of thyroid nodules has become the standard and the preferred technique for reasons of safety, cost, and efficacy.
Patients on Anticoagulation Therapy
The presence of a severe, uncorrected bleeding, platelet, or coagulation disorder rendering the patient incapable of hemostasis is an absolute contraindication for any type of a thyroid needle biopsy. In most patients receiving aspirin, warfarin (with possible exception of very high INR), heparin, or clopidogrel, it is safe to perform UGFNA of thyroid nodules and cervical lymph nodes using 25 or 27G needles without an increased risk of hematoma [18]. Similarly, it is not necessary to withhold novel oral anticoagulants (dabigatran, rivaroxaban, or apixaban) prior to performing UGFNA [19]. Additionally, anticoagulation therapy is not likely to result in a higher rate of inadequate cytology [20]. However if a prior FNA was inadequate on anticoagulation, it may be useful to withhold anticoagulation prior to repeat FNA [21].
For patients on anticoagulants, it is recommended to hold pressure for 5–10 min following the procedure and then check with ultrasound to see if a hematoma is forming. If so, this situation is managed by manual tamponage, followed by a pressure-taped dressing and/or an ice pack. The patient should be observed by ultrasound to assure stabilization prior to departure. The individual physician operator’s judgment and experience in performing UGFNA in these situations of a potentially increased risk of minor side effects is most important. Full disclosure of risks to the patient is mandatory prior to proceeding with UGFNA. Occasionally for UGFNA, withholding or reducing anticoagulation or other therapies may be appropriate. If there is a decision to defer the procedure or hold anticoagulation therapy, the referring or treating physician should be contacted.
Materials
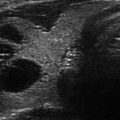
The ultrasound laboratory should consist of an ultrasound machine with a probe and linear transducer that has a 3.5–5.0 cm footprint and multiple frequency settings ranging between 7.5 and 14 MHz. The machine should also have Doppler imaging capabilities not only for diagnostic evaluation but also to identify blood vessels in the planned needle path (Fig. 12.1).

Figure 12.1
Left panel shows a transverse view (B-mode and power Doppler) with pressure applied on the transducer, masking the anterior jugular vein which is easily seen on the right panel (arrow) when less pressure is used. It is important to identify such blood vessels in order to avoid hematomas and bruising
Larger footprint transducers are cumbersome and may impede biopsy capabilities. An additional utility probe with a similar or lower frequency range is a 2 cm curvilinear or curved linear array transducer (a linear transducer with a convex-curved footprint that produces an image with an increased field of view in a sector format). The smaller curvilinear transducer footprint is useful for imaging and performing an FNA in difficult locations, especially in the lower neck region at the level of the manubrium, clavicles, and insertions of the sternocleidomastoid muscle (Fig. 12.2).

Figure 12.2
From left to right demonstrates different footprint sizes, linear array transducers with the transducer on the right demonstrating a smaller, curvilinear array transducer)
Additional items may include a mobile ultrasound machine, setup tray/cart, and patient imaging table or gurney, each of which can be easily moved for optimum positioning, visualization, and utilization during an UGFNA (Fig. 12.3). A second monitor placed across the imaging table allows the operator to visualize the UGFNA procedure without turning his/her head (Fig. 12.4). The setup tray should include all materials required for topical cleansing, as well as transducer covers, sterile coupling gel, and an assortment of needles readily assembled and accessible to perform UGFNA (Figs. 12.5 and 12.6). Small needles (25–27G), medium needles (21–23G), and specialty needles (25, 23, or 21G stylet-type needles or spinal needles) of variable lengths and types should be part of the routine setup (Fig. 12.2). Shorter (1/2–1 in.) needles can be used for small isthmus nodules to avoid the trachea. The stylet-type needles are used for deep nodules or for aspirating structures posterior to the thyroid, which may or may not lie within the thyroid (e.g., exophytic thyroid nodule vs. parathyroid tumor or lymph node). The stylet can be left in while advancing the needle preventing the uploading of thyroid cells into the needle prior to reaching the target. The stylet also stiffens the needle, making it easier to maneuver prior to withdrawing the stylet when in the nodule and performing an aspirate. A detachable needle guide adapted for the transducer or transmitted on the monitor screen in a biopsy mode setting on some ultrasound machines may be utilized if desired but usually is not necessary for routine UGFNA. These devices can be helpful in the FNA of deep or posteriorly located nodules and in performing specialized and prolonged procedures such as drainage of a large cyst followed by percutaneous ethanol injection. Almost any needle will be visible on modern high-resolution ultrasound equipment, and this makes use of echogenic needles unnecessary.

Figure 12.3
(a) UGFNA with assistant holding probe and monitor positioned for optimal viewing. (b) US-guided drainage of a large cyst with sonographer holding and adjusting the transducer, another assistant draining with large syringe via three-way stopcock, allowing physician to manipulate the large-bore needle to optimize complete drainage
Figure 12.4
Room setup: Position the monitor so that it is in clear view during the UGFNA
Figure 12.5
Various needle gauges and lengths as well as extension tubing should be available
Figure 12.6
Basic setup tray: 27 g 1¼” needles on 10 cc syringes (plunger pulled back 1–2 cc), alcohol prep pads, gauze, probe cover, sterile gel (optional as alcohol can serve as coupling agent), and bandage
For aspiration technique, a 3–10 cc syringe is connected to the needle. Pistol grip holders are not recommended since they are cumbersome and often apply excessive negative aspiration pressure, inducing bleeding and poor aspirates. However, these pistol grip holders can be used by an assistant in the drainage of a large cyst (Fig. 12.7).
Figure 12.7
Pistol grip syringe holder connected to large syringe and needle with extension tubing. The operator controls the needle under ultrasound guidance, and the assistant applies negative pressure using the pistol grip
The use of injectable or topical anesthesia is optional for a 27 or 25G needle procedure. The operator may choose to use one or more of the following for local anesthesia: injectable 1 or 2% lidocaine or, less commonly, ethyl chloride topical spray or a topical lidocaine gel or patch (applied 1 or 2 h prior to the procedure), or ice. Injectable lidocaine should be readily available pending the patient’s or physician’s preference; or the perceived need of a procedure that is technically difficult (e.g., involving multiple nodules or repetitive aspirations) or if a larger gauge needle is required for cyst drainage.
Technique
The patient should be positioned supine with the neck extended and soft pillow or pad inserted beneath the shoulders to optimize extension of the neck. An additional, small, soft pillow may be placed behind the head for patients who have known neck problems or discomfort with extension of the head and/or rotation of the extended neck. Based on prior knowledge of the planned procedure, the operator should position oneself on either side of the table or at the head of the table for optimal target lesion access during the performance of the aspiration procedure (Fig. 12.8). The neck can be rotated slightly toward the side of the nodule to avoid the sternocleidomastoid muscle by moving it laterally. The monitor should be clearly visible to the operator/physician during the entire procedure. Prior to prepping the neck, an extended field of view should be performed before every needle biopsy. Both lobes of the thyroid, the isthmus, low central region, and the lateral neck should all be observed for any abnormalities or lymphadenopathy not previously detected. Coupling gel is applied to the transducer face, and the transducer is then enclosed in a cover or Parafilm to avoid direct contact with any blood products. UGFNA is a clean but not sterile procedure—similar to phlebotomy. The covered transducer is cleaned with alcohol, and the neck area is prepped with alcohol swabs. Sterile coupling gel can be applied to the covered transducer face or directly to the prepped neck area. Alternatively the alcohol swab may serve as a coupling agent then reapplied between passes. This eliminates the possibility of contaminating the sample with gel.
Figure 12.8
Three different approaches for parallel technique: Cranial-caudal, trans-isthmus, and lateral
The key to utilizing ultrasound guidance for performance of the FNA is understanding the orientation of the azimuthal plane , which is the very thin plane in the middle of the transducer face along which the transducer sends and receives high-frequency ultrasound waves. Utilization of the azimuthal plane during UGFNA imaging allows the operator to visualize the needle pathway or approach, adjust the needle insertion angle, and track the entire needle and bevel-up tip by a parallel approach. Alternatively, the needle can be introduced perpendicular to the azimuthal plane, but in this orientation, only the bevel-up tip of the needle will be visible as it crosses the azimuthal plane (Fig. 12.9). Thus, there are basically two approaches for performing the UGFNA based on orientation to the azimuthal plane. The procedure may be done with an assistant holding the probe or with the operator holding the transducer in one hand and needle in the other (Figs. 12.3 and 12.10). A suggested step-by-step protocol is provided below.