Ultrasound of Muscle Injury
Introduction
Technique
The presence of bruising is important; the site of muscle damage frequently lies immediately proximal to the site of subcutaneous ecchymosis.
The sonologist should use the highest-frequency probe to give sufficient depth of penetration to allow assessment of the entire muscle under interrogation. In general high-frequency linear array probes (for example, 7–13 MHz and 5–17 MHz) can be used to assess muscle injury even in large compartments such as the thigh or hamstring. This is achieved by a combination of lowering the frequency of the probe to give sufficient penetration and by using electronic curvilinear field of view to give greater tissue coverage. Extended field of view scanning is useful in muscle ultrasound as it gives the examiner an appreciation of the overall muscle architecture and the degree of damage present. This is different to the use of extended field of view scanning in other areas where frequently it is only of value in demonstrating abnormalities for clinicians; in muscle ultrasound it helps with the grading and identification of muscle tears.
Muscle Anatomy
Muscle has a hierarchical internal structure with hypoechoic myofibrils separated by thin internal septa. This structure produces the typical ultrasound appearances of muscle tissue with hypoechoic tissue separated by thin hyperechoic parallel lines. This parallel orientation of the myofibrils renders muscle anisotropic, resulting in differing ultrasound properties dependent on the incident angle of the ultrasound beam. In transverse this produces the classic starry sky appearance with bright septa seen as dots within the hypoechoic dark surrounding myofibrils (Fig. 33.1). The echogenicity of the surrounding myofibrils varies with probe angle, either accentuating or decreasing this appearance. When examined in the longitudinal plane, muscle anisotropy is easier to appreciate by angling the probe or beam steering (Fig. 33.2). Within any single muscle there are usually separate functional bundles, especially in large muscles crossing two joints more prone to injury. This results in fibres tracking in different directions within muscles themselves, complicating even further the ultrasound assessment of muscle.
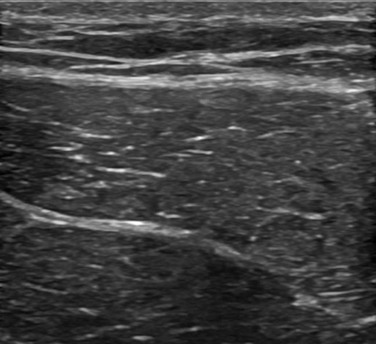
Figure 33.1 Transverse sonogram of the rectus femoris showing the typical starry sky appearance of the muscle septa with the surrounding myofibrils.
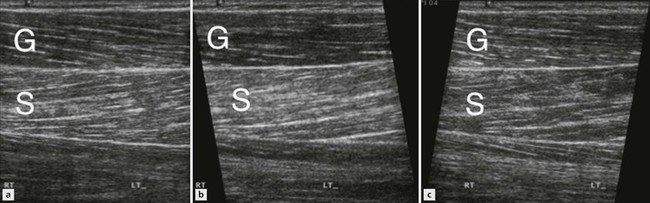
Figure 33.2 Image of the gastrocnemius (G) and soleus (S) muscles of the calf. With no beam steering (A) the gastrocnemius is slightly hypoechoic relative to soleus. Beam steering towards the feet accentuates this (B), whereas cranial beam steering (C) placed the gastrocnemius fibres more parallel to the probe, rendering them virtually isoechoic to the soleus fibres.
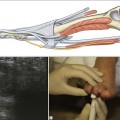
An understanding of myotendinous junction (MTJ) anatomy is vital to successful imaging of muscles (Fig. 33.3).
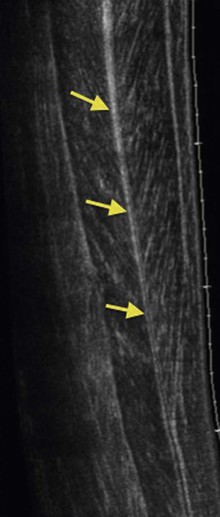
Figure 33.3 Extended field of view sonogram of the forearm demonstrating the long-central MTJ (arrows) in a bipennate muscle.
The junction between a muscle and a tendon can be either epimysial (at the periphery of the muscle) or via a central aponeurosis with a gradual thickening of the aponeurosis/epimyseum as the rounded tendon forms.
Anatomy of Commonly Injured Muscles
Quadriceps Anatomy
Rectus femoris crosses two joints and contains a high proportion of fast twitch fibres, which is why it is the most commonly injury of the knee extensors during kicking injuries.
This muscle also contains differing functional units with unipennate direct and bipennate indirect components that predispose to longitudinal splitting type of aponeurotic injury most commonly seen in the central septum.
Hamstring Anatomy
The hamstrings consist of three muscles, all of which cross two joints with high proportions of fast twitch fibres. Like rectus femoris, this combination makes them extremely prone to exercise-related injury. These muscles all arise from the ischial tuberosity.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


