CHAPTER 9
Univentricular Heart
Definition
The diagnosis and study of the univentricular heart is a complex issue, given the debate over the definition. This would seem to be an easy task on the basis of the simple name, “univentricular,” indicating one ventricle. A straightforward definition such as a univentricular heart is a three-chambered organ composed of two atria and one ventricle connected by one or two atrioventricular valves (cor triloculare biatriatum)1 is a good starting point. It is also generally agreed that the atrioventricular (AV) connection is central in defining the univentricular heart in which a single, double, or common inlet may exist. However, the controversy stems from the morphologically heterogeneity present and that recognition that truly solitary ventricles are quite rare. The complexity of these lesions has prompted debate over which abnormalities should be included in the univentricular heart syndrome; the debate continues.2–7
In general, it is agreed that only one functional ventricle is present within the ventricular mass. Often there is also an incomplete, rudimentary, or hypoplastic ventricle that lacks an AV connection. Only the well-developed ventricular chamber receives inflow from the atria through one or two AV valves and has an outlet portion to a great artery. The physiological result is that the systemic and pulmonary circulations are arranged in parallel fashion rather than in series as in the normal heart.8 The nomenclature debate focuses primarily on whether hearts with atretic tricuspid or mitral valves should3,4,6 or should not2,5 be included in the univentricular heart syndrome.
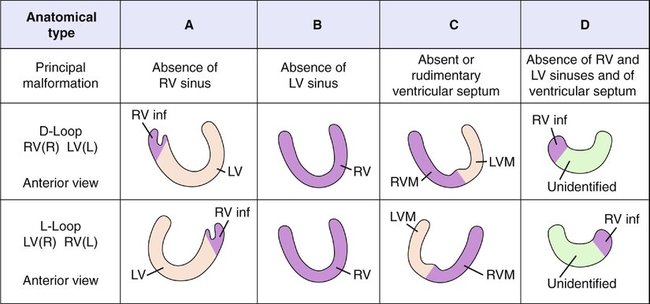
The classic and most commonly used description follows Hallermann’s modification of Van Praagh’s classification, in which one or two AV valves empty into a single ventricle.2 Van Praagh used the terms “single,” “common,” and “univentricular” interchangeably in his description. Tricuspid and mitral valve atresias are specifically excluded from this definition of the univentricular heart complex. Van Praagh’s classification system is depicted in Figure 9–1 and is described in detail further on.
If a broader definition is used, namely, that all atrial input goes into one ventricle, other anatomical abnormalities not originally included in Van Praagh’s classification can be considered.3,4 A classification scheme relevant to surgery was proposed by Jacobs in which a “single ventricle” was characterized as lacking two well-developed ventricles. Hypoplastic left heart was recognized as a common form of univentricular heart but was classified independently. The proposed definition encompassed double inlet AV connections, absence of one AV connection (mitral or tricuspid atresia), common AV valve and only one well-developed ventricle, and only one well-developed ventricle and heterotaxy syndrome, which describes a constellation of defects characterized by malposition of cardiac and abdominal visceral structures. By these criteria, univentricular heart becomes a broader category of congenital malformations characterized by both atria relating entirely or almost entirely to one functionally single ventricular chamber.7,8 This new scheme incorporated aspects of both Van Praagh’s and Anderson’s classification systems.
Anderson et al3 stressed that “univentricular heart” should include the tricuspid and mitral atresias because the primary definition for univentricular heart was satisfied regardless of whether one of the AV valves was absent or atretic. Although the debate continues, most authors still separate the valve atresias from univentricular heart complex as a matter of tradition.2,5,9–13 However, the classification of Anderson et al is helpful when trying to understand the embryological and anatomical characteristics of the univentricular heart syndrome, which is described with that of Van Praagh further on.
Embryology
A univentricular heart is thought to be caused by failure of development at the bulboventricular loop stage.15 At this stage, the bulbus cordis moves ventrally and to the right of the common ventricle. The folding of the heart tube causes a spur to be formed, the bulboventricular spur. It projects between the common ventricle and the bulbus cordis and is normally absorbed into the ventral wall of the ventricle. At the same time, the bulbus cordis shifts and grows to the left to form the right ventricle and the muscular portion of the interventricular septum. If developmental arrest occurs at this stage, the morphological characteristics of a single ventricle result.
The hemodynamic consequences of developmental arrest (i.e., decreased or obstructed blood flow) result in other findings associated with single ventricles, such as rudimentary chambers and great vessel abnormalities.16
Anatomy
To understand the anatomy of univentricular heart disease, it is useful to review the classification schemes that have been proposed.2,3 The Van Praagh classification of the univentricular heart is detailed and particularly useful for cardiac surgeons, but it is complex.
According to Hallermann’s modification of the Van Praagh classification2 depicted in Figure 9–1, the ventricle is designated by the letters A, B, C, or D, depending on whether the morphological characteristics are left, right, a combination of left and right, or indeterminate and depending on whether a left or a right sinus (rudimentary chamber) is present.
Note that the position of the great vessels is determined at the level of the semilunar valves. The most common type of univentricular heart diagnosed in children is Van Praagh’s A3, accounting for nearly 60% of cases.2,9
In one series of affected children diagnosed between the ages of 4 and 10 years at the Mayo Clinic,9 67% of lesions were type A and 16% were type C. However, selection bias occurred in this sample because diagnoses were generally made later in childhood and the patients represent a subset who had survived past infancy with univentricular hearts. Therefore these data do not include neonates and infants with early-onset symptoms resulting from more severe, life-threatening lesions and may be skewed toward type A ventricles.
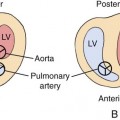
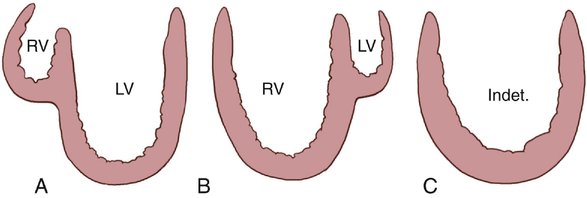
The univentricular heart categorization of Anderson et al3,4 is helpful because it simplifies the anatomical variations in the univentricular heart syndrome diagrammatically. These authors stress that univentricular heart means a main ventricular chamber with morphological characteristics of the left or right ventricle or indeterminate characteristics, with or without a rudimentary chamber within a single ventricular mass (Fig. 9–2). Left ventricles have relatively smooth walls, fine trabeculations, and lack septal chordal attachments of the AV valve. In contrast, right ventricles are more coarsely trabeculated and commonly have chordal attachments of the AV valve to the septal surface.7
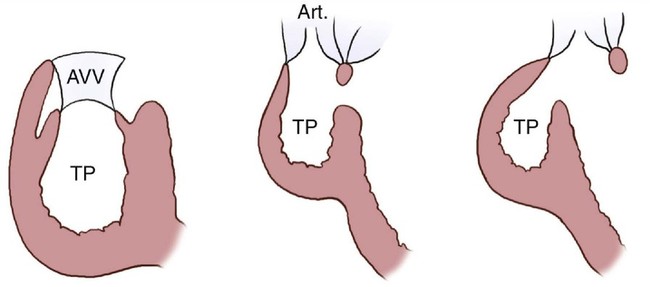
The ventricle and the rudimentary chamber most commonly have discordant morphological features, that is, a left ventricle with a right rudimentary chamber. By definition, the rudimentary chamber does not have an inlet, but it may have an outlet. If the chamber does have an outlet and supports a great vessel, it is called an outlet chamber; if not, the term trabecular pouch is used (Fig. 9–3).