and Arumugam Rajesh2
(1)
Department of Radiology, Harvard Medical School Massachusetts General Hospital, Boston, Massachusetts, USA
(2)
Department of Radiology, University Hospitals of Leicester NHS Tr Leicester General Hospital, Leicester, UK
Case 3.1
Brief Case Summary:
35 year old male with abdominal pain
Imaging Findings
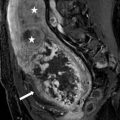
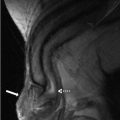
CT urogram (excretory phase) of the abdomen demonstrates the right ureter lying posterior to the inferior vena cava (Fig. 3.1). Coronal reconstructed image demonstrates the presence of an abrupt narrowing of the ureter at this level (arrow, Fig. 3.2).


Fig. 3.1
CT urogram (excretory phase) of the abdomen demonstrates the right ureter (arrow) lying posterior to the inferior vena cava
Fig. 3.2
Coronal reconstructed image demonstrates the presence of an abrupt narrowing of the ureter at this level (arrow)
Differential Diagnosis
Retrocaval ureter, medial deviation of the ureter related to retroperitoneal fibrosis.
Diagnosis and Discussion
Retrocaval ureter.
A retrocaval ureter is an uncommon congenital anomaly with an incidence of 1:1,000. The etiology is related to abnormal development of the inferior vena cava (IVC), and not the ureter itself, resulting in a portion of the ureter passing behind the IVC. It is seen slightly more commonly in males (two to three fold increase) and typically occurs on the right side. Symptoms include intermittent pain related to ureteral obstruction as well as hematuria.
While imaging findings were first described with conventional urography and intravenous pyelography (IVP), both CT and MRI are used currently to diagnose this entity. Two subtypes have been described. Type 1 (or “low loop” form) manifests with the ureter passing behind the IVC at the level of the third or fourth vertebral body resulting a “reverse J” (also described as an “S” shape or “fish hook” deformity) configuration of the ureter at the point of transition. In the type 2 (or “high loop” form) subtype, the ureter passes behind the IVC at the level of or just above the ureteropelvic junction, resulting in a sickle shape at the point of transition. Type 1 is more common and is associated with higher degrees of ureteral obstruction.
Symptomatic patients or those with moderate to severe hydronephrosis are evaluated for surgical correction which involves ureteral transection with placement of the affected ureteral segment anterior to the IVC. Treatment has traditionally been via an open surgical technique, though laparoscopic reconstructive techniques are being increasingly used with favorable outcomes.
Pitfalls
The differential diagnosis for medial deviation of the ureter on IVP includes retroperitoneal fibrosis, a retroperitoneal mass or prior surgery. Definitive findings can be established using either a CT or MRI urogram protocol.
Teaching Points
1.
Retrocaval ureter is a congenital abnormality which results in the ureter passing posterior to the IVC. The embryological anomaly is related to development of the IVC and not the ureter.
2.
Two types exist. Type 1 is more common and results in worsening degrees of ureteral obstruction. Both types result in the ureter passing posterior to the IVC. In type 1, this transition occurs at the level of mid lumbar spine giving rise to a “reverse J”, “S” shape or “fish hook” deformity. In type 2, the transition occurs at or above the level of the ureteropelvic junction resulting in a sickle shape appearance of the ureter.
3.
Surgery is reserved for symptomatic patients or those with moderate to severe hydronephrosis
Case 3.2
Brief Case Summary:
45 year old male with hematuria.
Imaging Findings
Conventional radiographs of the abdomen obtained as part of a retrograde urogram demonstrate the presence of multiple small filling defects in the left proximal ureter (arrows in Figs. 3.3, 3.4, and 3.5). The bladder is filled with contrast and a small amount of contrast is noted in the right mid to distal ureter.



Fig. 3.3
Conventional radiograph of the abdomen obtained as part of a retrograde urogram demonstrating the presence of multiple small filling defects in the left proximal ureter (arrow)
Fig. 3.4
Conventional radiograph of the abdomen obtained as part of a retrograde urogram demonstrating the presence of multiple small filling defects in the left proximal ureter (arrow)
Fig. 3.5
Conventional radiograph of the abdomen obtained as part of a retrograde urogram demonstrating the presence of multiple small filling defects in the left proximal ureter (arrow)
Differential Diagnosis
Transitional cell carcinoma, blood clots, ureteral stones, ureteritis cystica.
Diagnosis and Discussion
Ureteritis cystica.
Ureteritis cystica is an uncommon benign process characterized by the formation of multiple epithelial lined submucosal cysts which protrude into the ureteral lumen. Histologically, the cysts are thought to represent cystic degeneration of invaginated epithelial cell nests. It is more commonly seen in older age groups and there is no gender predilection. Clinically, patients with ureteritis cystica usually have evidence of chronic urinary tract inflammation (such as a history of recurrent urinary tract infections) and may present with hematuria.
Conventional or CT urographic examinations are the imaging studies of choice. Ureteritis cystica typically presents as multiple small (often less than 5 mm), smooth filling defects which can, on occasion, given the ureter a scalloped appearance. The filling defects can be seen throughout any portion of the excretory system. Within the ureter, they can be unilateral or bilateral, though there is a predilection for the upper third. Urinary tract dilatation without hydronephrosis may be observed.
The imaging findings are often non-specific, with uroepithelial malignancy being the most important mimicker. Urological evaluation with consideration of ureteroscopy is usually warranted when the imaging features are inconclusive. Treatment is conservative and is directed at treating the cause of inflammation. The imaging appearance may regress or remain stable after the cessation of treatment. There is no definite increased risk for developing an uroepithelial malignancy.
Pitfalls
Ureteritis cystica is included in the differential diagnosis of ureteral filling defects, along with transitional cell carcinoma, blood clots, and stones. Some of these mimickers can be excluded using a combination of the clinical information and the use of CT urographic imaging. The non-contrast portion of the exam allows evaluation for stones and blood clots, while the nephrographic and excretory phase images allows for the evaluation of enhancing soft tissue tumors. If imaging findings remain inconclusive, ureteroscopy should be considered.
Teaching Points
1.
Ureteritis cystica is a benign condition characterized the presence of submucosal ureteral cysts which protrude into the lumen, manifesting radiographically as multiple filling defects. It is associated with conditions that promote chronic inflammation.
2.
The most important differential diagnosis for ureteral filling defects is transitional cell carcinoma. A combination of clinical and CT urography findings can help make this distinction. A ureteroscopy should be considered to evaluate the entire urothelial system including the bladder and ureters for transitional cell carcinoma.
3.
Treatment is aimed at managing the underlying cause of inflammation. Imaging findings may remain stable or improve following treatment. There is no definite increased risk for developing an uroepithelial malignancy.
Case 3.3
Brief Case Summary:
47 year old male with hematuria
Imaging Findings
Reconstructed coronal image from an excretory phase of a CT urogram demonstrates the presence of multiple outpouchings involving the mid portions of both ureters (arrows, Fig. 3.6). 3D reconstructed images shows the same findings (Fig. 3.7).

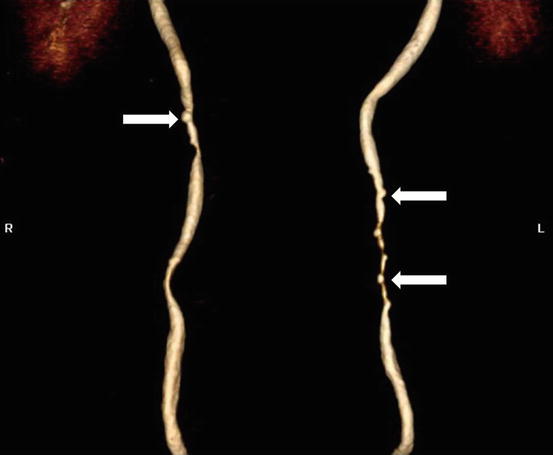
Fig. 3.6
Reconstructed coronal image from an excretory phase of a CT urogram demonstrates the presence of multiple outpouchings involving the mid portions of both ureters (arrows)
Fig. 3.7
3D reconstructed images demonstrates multiple outpouchings of the mid ureters (arrows)
Differential Diagnosis
Ureteral pseudodiverticulosis, ureteritis cystica, tuberculosis ureteritis, ureteral diverticula
Diagnosis and Discussion:
Ureteral pseudodiverticulosis
Ureteral pseudodiverticulosis (UP) is typically an incidental finding seen in the workup for urinary symptoms. Histologically, UP represents a protrusion of hyperplastic transitional epithelium into the subepithelial connective tissue, typically in the background of underlying inflammation. The incidence is approximately 11 %.
Traditionally, UP has been diagnosed on conventional anterograde or retrograde urography studies where it is defined by multiple small ureteral outpouchings, measuring less than 4 mm. The lesions are often bilateral and commonly involve the mid to upper one-third of the ureter. If unilateral, UP is more commonly seen in the left ureter. There may be some mild narrowing of the associated ureteral segment. CT urography, which has largely replaced conventional anterograde urography for the evaluation of the upper urinary tracts, demonstrates similar findings, best appreciated on coronal reconstructed images.
While UP is a benign lesion, it is associated with an increased risk for uroepithelial malignancy. While this risk has been traditionally quoted as 25 %, further studies by Wasserman et al. suggest a higher association reaching up to 71 % if UP is seen with radiolucent filling defects or strictures. The most common associated malignancy is transitional cell carcinoma, though squamous cell carcinoma has been reported. There is no known association between the number of outpouchings and the risk of malignancy and all cases should be closely monitored.
Pitfalls
The appearance of UP is fairly pathognomonic on imaging studies. True diverticula of the ureter are exceedingly rare and usually present as a single large lesion. Histologically true diverticula of the ureter involve all the layers of the ureteral wall. Ureteritis cystica manifests as filling defects rather than focal small outpouchings. Tuberculosis ureteritis has a variety of imaging appearances but is usually associated with papillary necrosis, strictures, and calcifications.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


