Anatomy, embryology, pathophysiology
- ◼
Urinary tract obstruction (UTO) is a commonly encountered clinical scenario that can affect all age groups. In the pediatric population, the underlying pathology is often congenital in nature ( Box 26.1 ), whereas in adults, there is a variety of acquired conditions ( Table 26.1 ). The site of obstruction may range from the renal hilum, along the course of the ureter, the bladder or the urethra.
Box 26.1
Embryological Anomalies Associated With Urinary Tract Obstruction
- ◼
Horseshoe kidney
- ◼
Ectopic kidney
- ◼
Ureteropelvic junction obstruction
- ◼
Duplicated ureter
- ◼
Ureterocele
- ◼
Ectopic ureteral insertion
- ◼
Retrocaval ureter
- ◼
Posterior urethral valves
Table 26.1
Acquired Urinary Tract Obstruction Listed by Location
Kidney/Renal Pelvis
Ureter
Bladder
Urethra
Staghorn calculus
Sloughed papilla
Ureteropelvic junction obstruction
Infundibular stenosis
Urothelial carcinoma
Calculus
Blood clot
Urothelial carcinoma
Stricture (sequela of infection, surgery or radiation therapy)
Ureterocele
Extrinsic compression
- ◼
Retroperitoneal fibrosis
- ◼
Retroperitoneal adenopathy
- ◼
Retroperitoneal abscess
- ◼
Aortic aneurysm
- ◼
Endometriosis
- ◼
Pregnancy
- ◼
Calculus
Urothelial carcinoma
Neurogenic bladder
Calculus
Stricture (sequalae of infection or inflammation)
Benign prostatic hyperplasia
Prostate carcinoma
Urethral carcinoma
- ◼
- ◼
Reviewing embryological development can help with understanding the scope of described congenital anomalies.
- ◼
The kidneys arise from the metanephros and develop in the pelvis before ascending into the abdomen. The metanephric system arises from the ureteric bud and forms the renal collecting system and ureter.
- ◼
The urogenital sinus is traditionally divided into two parts. The ventral/pelvic portion forms the bladder and entire female urethra or part of the male urethra. The urethral portion forms the male penile urethra or lower part of the vaginal vestibule in females.
- ◼
The mesonephric ducts (normally form part of the male ejaculatory system and regress in females) are closely related to the caudal end of the ureteric bud. The ureteric buds separate from the mesonephric ducts and fuse independently with the urogenital sinus.
- ◼
- ◼
The definition of UTO is any process that results in impeded urine flow and increased upstream collecting system pressure. An important point is that UTO may or may not lead to upstream dilation. The converse statement is also true: a dilated collecting system is not always a result of UTO.
- ◼
Pathophysiology: the inciting event is a disease process resulting in UTO. What follows is a complex pathophysiological course that begins with increased collecting system pressure resulting in increased resistance to renal blood flow. This ultimately leads to renal parenchymal ischemic changes and corticomedullary atrophy (irreversible loss of nephrons).
- ◼
The process may be reversible depending on the length and degree of obstruction, although complete obstruction more than 24 hours usually leads to some level of permanent loss of renal function.
- ◼
In the acute phase, the kidneys may appear enlarged. The papilla of the medullary pyramids may appear blunted and over time become cupped. There can be minimal to marked dilation of the renal collecting system and ureter to the level of obstruction. Chronically, there will be renal cortical thinning.
- ◼
Techniques
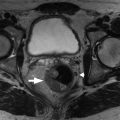
Various grading systems exist for describing the degree of hydronephrosis. The most widely used grading system was created by the Society for Fetal Urology (SFU; Table 26.2 ) and in some fashion is routinely applied in adults with mild, moderate, and severe hydronephrosis correlating to grade I, grade II, and grade III, respectively. Grade IV includes renal parenchymal thinning ( Fig. 26.1 ), which is an important finding to report although is nonspecific and can be seen with varying grade of hydronephrosis in adults. Grading hydronephrosis across imaging modalities depends on a visual assessment of the kidney and collecting system and is inherently susceptible to a degree of subjectivity. Other systems have been proposed, including a quantitative assessment described as the hydronephrosis index (HI), which has shown good correlation with the SFU grading system with less subjectivity, but is rarely used in most clinical radiological practices (Krishnan, 2009).
| Grade | Imaging Appearance |
|---|---|
| I | Splitting of central renal complex without calyceal involvement. Normal renal parenchyma. |
| II | Splitting of central renal complex with filling of intrarenal pelvis and fluid extending to nondilated calyces. Normal renal parenchyma. |
| III | Dilated intrarenal pelvis beyond renal sinus extending into uniformly dilated calyces. Normal renal parenchyma. |
| IV | Same as grade III except with renal parenchymal thinning. |

Plain film
- ◼
Overall, provides a limited scope of information but may have clues to etiology. Up to 90% of urolithiasis is reported visible on radiography although the mere presence of urinary calculi does not signify obstruction. Imaging can be limited by stone size, patient body habitus, as well as extraurinary calcifications (see Chapter 22 ).
Intravenous pyelography
- ◼
Brief overview of key imaging findings in setting of acute UTO:
- ◼
Delayed immediate nephrogram, as well as progressive increasing density of nephrogram.
- ◼
Delayed contrast excretion into the collection system.
- ◼
Variable hydroureteronephrosis to the point of obstruction.
- ◼
- ◼
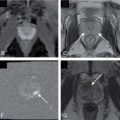
Intravenous pyelography (IVP) in the setting of chronic UTO may show delayed nephrogram, renal atrophic changes, as well as delayed contrast excretion ( Fig. 26.2 ).