Abstract
The urinary tract is one the most difficult organ systems of the body to evaluate on FDG PET/CT. This is because of physiologic excretion of FDG through the kidneys, ureters, and bladder. FDG in urine may hide FDG-avid malignancy or be mistaken for FDG-avid malignancy. Careful attention must be paid to both the FDG PET and CT components of an FDG PET/CT to prevent mistakes. The differential for solid renal masses includes RCC, oncocytoma, TCC, and AML, lymphoma, and metastases. The presence of macroscopic fat on CT is usually diagnostic of AML. TCC arise from the collecting system epithelium and are usually centered along this epithelium. It is usually not possible to distinguish RCC and oncocytoma on imaging, and thus pathology is usually necessary. All of these lesions have variable FDG avidity which may be obscured by FDG in adjacent urine.
Keywords
FDG, PET/CT, kidney, ureter, bladder, renal cell carcinoma, oncocytoma, transitional cell carcinoma, bladder cancer
The urinary tract is one the most difficult organ systems of the body to evaluate on F18-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT). This is because of physiologic excretion of FDG through the kidneys, ureters, and bladder. FDG in urine may hide FDG-avid malignancy or be mistaken for FDG-avid malignancy. Combine this with the fact that neoplasms of the urinary tract are often only mildly FDG avid, and you can see why careful attention must be paid to both the FDG PET and CT components of an FDG PET/CT to prevent mistakes.
Kidney
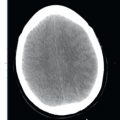
There are two paired kidneys in the retroperitoneum of the abdomen. However, there are multiple congenital anomalies which result in an unexpected location or absence of a kidney. These congenital anomalies should be recognized on FDG PET/CT images to prevent misinterpretation. In a case of renal agenesis, only one kidney will be visualized on the FDG maximum intensity projection (MIP) and cross-sectional images. With a horseshoe kidney, the kidneys will be fused in the midline. As opposed to normal separate kidneys which normally lie superomedial to inferolateral, the inferior poles with a horseshoe kidney will be directed medially ( Fig. 18.1 ). Crossed fused renal ectopia is a less common congenital anomaly where the kidneys are fused and lie on one side of the spine ( Fig. 18.2 ). With crossed fused renal ectopia there will be two collecting systems and two ureters arising from the fused kidney.


Renal masses have a different differential diagnosis depending on whether they are solid or cystic. The differential diagnosis for solid renal masses includes primary renal neoplasms (renal cell carcinoma [RCC], oncocytoma, transitional cell carcinoma [TCC], angiomyolipoma [AML]), as well as renal lymphoma and renal metastases. In children, solid renal masses are uncommon, but when they occur they are most often Wilms tumors. Cystic renal masses include simple cysts, complicated cyst, multilocular cystic nephroma, cystic RCC, and renal abscesses/infections.
Renal Cell Carcinoma
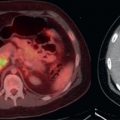
The majority of solid renal masses in adults are RCC. There are multiple histologic subtypes of RCC, the most common being clear cell carcinoma, with the majority of the remainder being papillary or chromophobe RCC. On CT, RCC may be hypointense, isointense, or hyperintense to normal renal parenchyma. Following intravenous contrast administration, RCC demonstrates variable intensities of enhancement, with clear cell subtypes usually enhancing more avidly. Hemorrhage, necrosis, and/or calcifications are common. On FDG PET, RCC ranges from markedly FDG avid to FDG avidity equal to background renal parenchyma. Even when an RCC is FDG avid, urine within the collecting system of the kidney may obscure the RCC. The RCC may be more apparent on CT images than on FDG PET, particularly if intravenous contrast has been administered. Sometimes, it is only an abnormality in renal contour or change in size of a renal mass which allows detection of RCC on FDG PET/CT ( Fig. 18.3 ). Because RCCs are increasingly being detected incidentally on imaging examinations, it is important to combined findings from the kidneys on both FDG PET and CT to prevent missing lesions. Metastases from RCC may be more FDG avid than the primary malignancy ( Fig. 18.4 ). RCC metastases are most commonly pulmonary and osseous, although any organ may be involved. Local nodal metastases in the retroperitoneum are also common. RCC may grow directly into the renal vein and then into more central veins. Expansion, enhancement, or FDG avidity in the local veins is suspicious for direct venous extension.


Oncocytoma
Oncocytoma is a benign solid renal tumor. Unfortunately, it is usually difficult to distinguish an oncocytoma from an RCC on imaging, thus tissue sampling is usually required to make the diagnosis. On CT, oncocytomas are usually isointense or hyperintense to normal renal parenchyma. Enhancement is common. The presence of a central stellate scar may suggest an oncocytoma, but this is not sufficiently accurate to rely upon. On FDG PET, oncocytomas demonstrate FDG avidity that varies from background renal parenchyma to markedly FDG avid, similar to RCC, and thus FDG PET cannot distinguish an oncocytoma from an RCC.
Transitional Cell Carcinoma
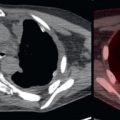
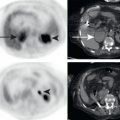
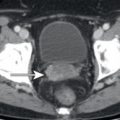
TCCs are malignant tumors of the renal collecting system epithelium. TCCs may be found in the kidneys, ureters, or bladder, with the bladder being the most common site. On CT, TCCs may be visualized as soft tissue masses causing a filling defect or distortion within the collecting system or the lumen of the ureter or bladder. Enhancement is usually mild. Calcifications are uncommon. On FDG PET, TCCs demonstrate FDG avidity that varies from background to marked FDG avidity. As TCCs occur in the lining of the collecting system, obscuration by FDG in urine is common, and thus comparison with the findings is essential for localizing these tumors. When the TCC is less FDG avid than FDG in the urine, CT findings may be the only evidence of the lesion ( Fig. 18.5 ). TCCs are known for drop metastases, with primary malignancies in the kidney collecting system resulting in drop metastases in the ipsilateral ureter or the bladder ( Fig. 18.6 ).


Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


