Trauma may be categorized as blunt, penetrating, or iatrogenic. In many patients, especially those with blunt trauma, the severity of injury is difficult to judge from the physical examination and imaging studies are obtained.
▪ RENAL INJURIES
Clinical Features
In most series, blunt trauma accounts for 80% of all renal injuries, but the incidence reported depends on the referral pattern of the reporting institution. Approximately three-fourths of the reported renal injuries occur in men younger than 50 years. Motor vehicle accidents account for about one-half of the reported cases; falls, altercations, industrial accidents, and sports injuries comprise the remainder.
Hematuria after blunt abdominal injury is common; significant injury to the kidney, however, is relatively uncommon. Most blunt renal injuries occur in patients suffering multisystem trauma. The liver and spleen are the abdominal organs most commonly associated with renal injury, followed by the pancreas, colon, and small bowel.
Penetrating renal injuries fall into two categories: (1) those related to gunshot wounds and (2) those related to stabbings. Hematuria after penetrating injury is virtually always a sign of renal damage that requires evaluation. Limited posterior stab wounds that do not penetrate the renal fossa are managed conservatively by many surgeons. In the remainder, the mere demonstration that the kidney is in the path of the injury or the presence of hematuria is an indication for surgical exploration. More than 80% of gunshot wounds of the kidney are associated with other abdominal injuries, usually of the bowel, pancreas, diaphragm, liver, or spleen.
Anatomy and Mechanism of Injury
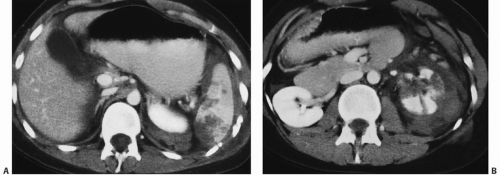
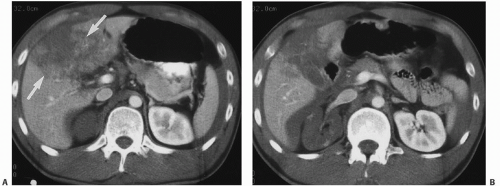
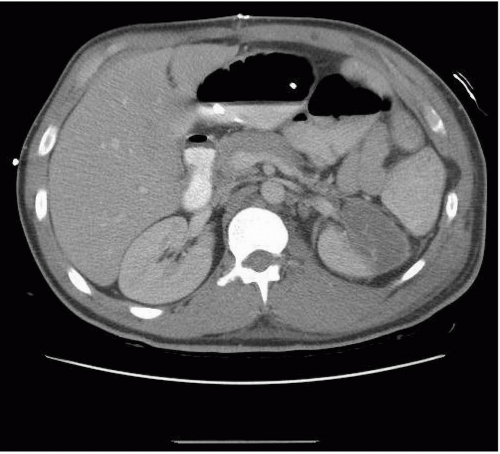
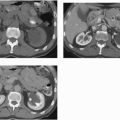
The kidney is relatively protected from injury by the rib cage, vertebral column, and psoas muscles. The fascial coverings of the kidney and the retroperitoneal fat provide additional protection. Injury of the lower ribs or vertebrae is associated with a higher incidence of renal injury; an injury to the spleen frequently accompanies injury to the left kidney (Fig. 21.1), whereas a liver injury often accompanies injury of the right kidney (Fig. 21.2). Bleeding from renal injuries is frequently self-limiting because Gerota fascia provides a tamponade effect.
Bleeding within the renal parenchyma results in an intrarenal hematoma. Bleeding that occurs between the renal parenchyma and the renal capsule is a subcapsular hematoma. If the capsule is also torn, hemorrhage confined by Gerota fascia is termed perinephric hematoma. Rarely, hemorrhage may extend beyond Gerota fascia into the retroperitoneum.
Blunt injuries of the kidney occur as a result of a direct blow to the flank or from deceleration. With a direct blow, the kidney is crushed, causing one or more lacerations of the renal parenchyma that result in intrarenal, subcapsular, or perinephric hematomas. With a deceleration injury, acute tension on the renal pedicle may produce a laceration of the renal vein or artery, an intimal tear in the vessel that often results in secondary thrombosis, or rarely laceration or avulsion of the ureteropelvic junction (UPJ).
In patients with a preexisting renal abnormality, relatively minor trauma may cause disproportionate symptomatology that brings the patient to medical attention. Such underlying conditions include calculi, tumors, cystic disease, and some congenital conditions, including UPJ obstruction and horseshoe kidney.
Penetrating injury usually results in direct injury of the renal parenchyma, vascular pedicle, or collecting system. Iatrogenic renal injuries may occur either from renal biopsy or from percutaneous nephrostomy placement; both may result in bleeding (subcapsular or perinephric hematoma) or in arteriovenous fistula formation.
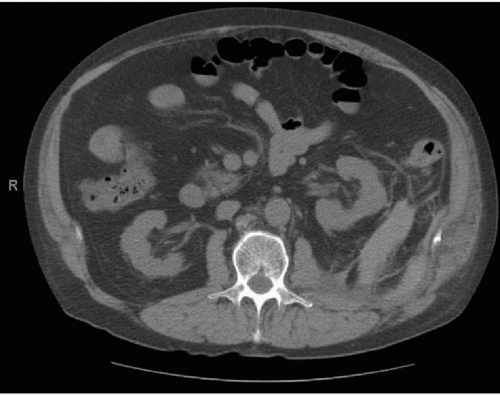
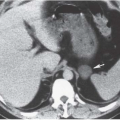
Traumatic injury may also be iatrogenic in etiology, as a complication of urinary tract intervention, as inadvertent injury during surgery, or as an invasive procedure (Fig. 21.3).
Diagnostic Approach to Imaging Renal Trauma
The imaging evaluation of suspected urinary tract injury depends not only on the types of injuries the patient has likely suffered, but also on the philosophy of the attending physicians and the equipment and support available. As a rule, evaluation of the lower urinary tract should precede evaluation of the upper urinary tract, when both are indicated. In male patients, urethrography should precede cystography. Since a computed tomography (CT) examination is often performed for other reasons, CT cystography may be used to evaluate possible bladder rupture.
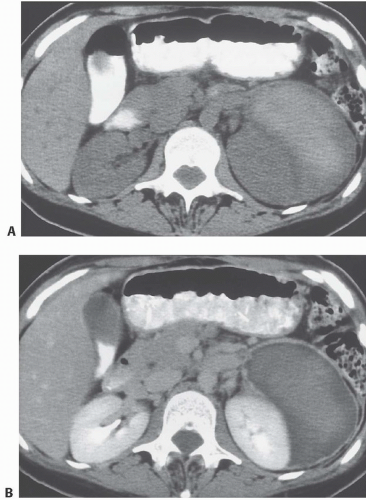
FIGURE 21.1. A: CT scan through the upper abdomen demonstrates multiple splenic lacerations. A small perinephric hematoma surrounding the upper pole of the left kidney is also seen. B: CT scan through the midportion of the left kidney shows multiple renal lacerations with a large perinephric hematoma.
There is diversity of opinion regarding the value of CT of the abdomen as a screening study for suspected intra-abdominal injury. Ultrasound (US) is used as the primary imaging examination in patients with blunt abdominal trauma in some centers in the United States and is more broadly used in Europe and Asia. It is portable and relatively inexpensive, avoids ionizing radiation, and does not interfere with ongoing resuscitation. However, the examination is limited by a large body habitus and the presence of gas, and the results are operator dependent.
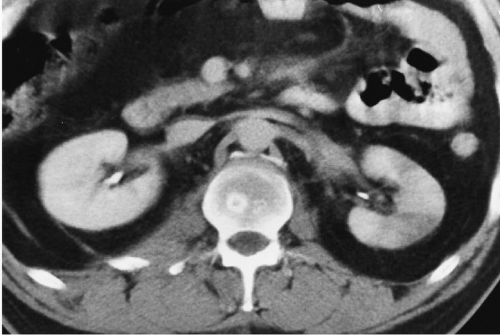
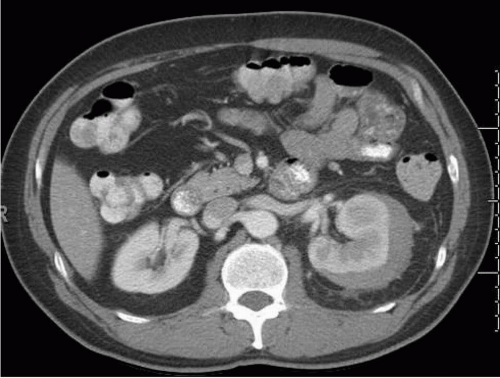
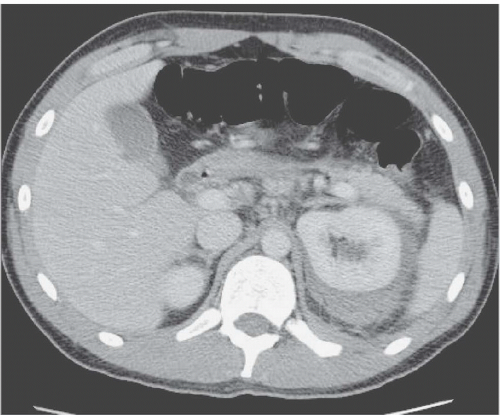
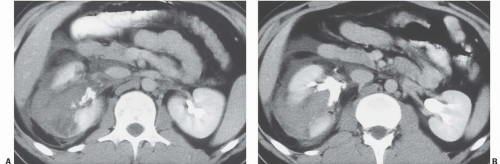
FIGURE 21.2. A: CT scan through the upper abdomen demonstrates a large liver laceration (arrows). B: CT section at the level of the kidneys demonstrates absent enhancement of the right kidney as a result of segmental renal infarction. A hemoperitoneum is also present.
If a screening US examination is positive, the patient undergoes a CT examination for further clarification. If the examination is negative, it is unclear whether a CT examination is needed. Sirlin et al. (2004) reported a true negative rate of 99.9% in a series of 4,000 patients having a screening US examination after blunt trauma. Despite these excellent results, abdomen and pelvic CT remains the most commonly used imaging examination in patients after blunt trauma. The continued advances in CT technology enable rapid assessment of the abdomen and pelvis at lower radiation doses than has been previously possible.
In patients who have suffered penetrating injury, CT should be performed as a first-line study. CT is commonly used to define the renal injury and to exclude an abnormality of the contralateral kidney.
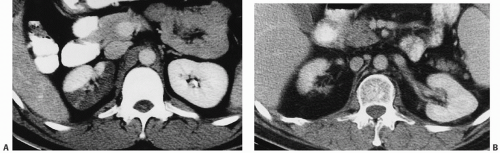
FIGURE 21.3. A small perinephric hematoma is seen as high-density blood after a renal biopsy.
Radiologic Examination
Computed Tomography
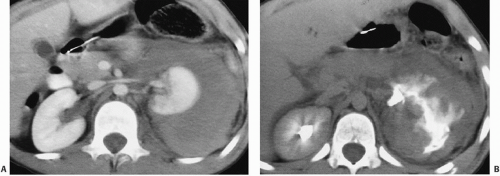
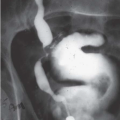
Multirow detector CT (MDCT) is routinely performed after the intravenous administration of 100 to 125 cc of iodinated, nonionic contrast media. Imaging is typically obtained 90 seconds after contrast media administration. Arterial phase imaging may be obtained if vascular injury is suspected, and delayed images can be obtained to image the renal collecting system and bladder, as indicated. Delayed scans are needed to visualize the collecting system (Fig. 21.4) if injury to the collecting system is suspected.
Ultrasound
An US examination of the abdomen may be used to detect intraperitoneal bleeding. Free fluid appears as a hypoechoic region most readily detected in the hepatorenal fossa, around the tip of the spleen or in the pelvis. Acute perinephric hematomas may be difficult to detect because echogenic blood in the retroperitoneum may be difficult to distinguish from echogenic perinephric fat. As hematomas liquefy, however, they become more readily visible. For this reason, US is useful to follow injuries that have been identified on CT in cases where it is desirable to limit radiation exposure to the patient. Thus, US is particularly useful in the evaluation of pregnant women and in the follow-up of renal injuries in children.
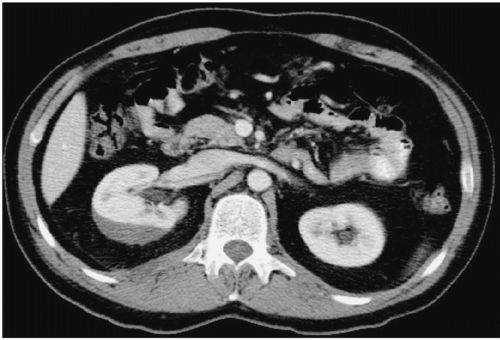
FIGURE 21.4. A: Nephrographic phase CT image shows a large amount of fluid surrounding the left kidney. B: An excretory phase image shows perinephric urinary extravasation from a laceration extending into the collecting system.
Magnetic Resonance Imaging
The role of magnetic resonance imaging (MRI) in trauma patients is limited, particularly in the acute setting. Follow-up imaging of documented acute injuries on CT may be performed in patients whose renal function has deteriorated sufficiently to preclude administration of iodinated contrast material. In the same setting, MRI may be used to assess the vascular integrity of the kidney and the integrity of the renal collecting system. However, the use of gadolinium contrast media in patients with renal failure is associated with nephrogenic systemic fibrosis. The ability to display images in both the sagittal and the coronal planes may also be of benefit in assessing the true extent of injury.
Angiography
The use of angiography in the evaluation of renal injuries has significantly declined with the increased use of CT, and is now used almost exclusively when vascular occlusion of actively bleeding vessels is contemplated.
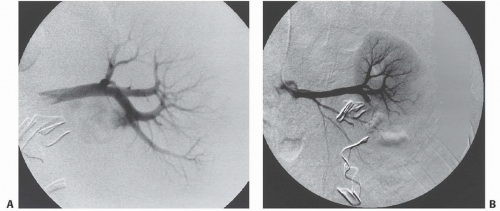
After penetrating trauma, angiography is used to identify traumatic lesions such as arteriovenous fistulae and pseudoaneurysms. Angiography provides a method by which traumatic renal hemorrhage can not only be diagnosed, but also directly be treated through transcatheter embolization (Fig. 21.5).
Classification
The American Association of Surgeons in Trauma classifies renal injuries into five grades (Table 21.1). Approximately 80% of injuries are grade I, which include parenchymal contusions and small subcapsular hematomas. The frequency with which more severe grades are seen is approximately 5% each. Renal injuries may also be classified according to the severity of the injury and the therapeutic implications. A system commonly used in radiology (Table 21.2) is described here.
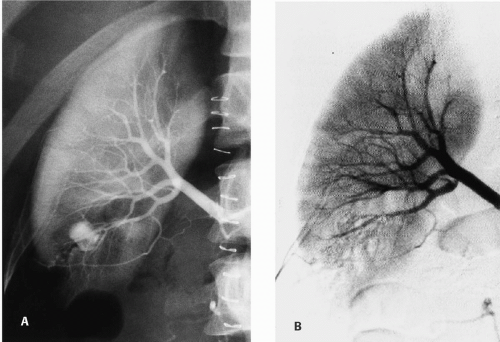
FIGURE 21.5. Traumatic renal hemorrhage. A: Arterial phase study shows frank bleeding from a laceration of a lower segmental artery. B: After embolization with Gelfoam (Upjohn, Kalamazoo, Michigan), the bleeding is controlled.
Minor Injuries
Minor injuries may be treated expectantly, and rarely require surgical intervention. They are the most common form of renal injury, comprising 85% of injuries in most series. In patients suffering isolated renal injuries, minor injuries constitute an even higher percentage of the injuries. In those suffering multisystem trauma, minor injuries still account for 75% of the total. The vast majority of minor renal injuries consist of small to moderate intrarenal hematomas that are also called renal contusions (Fig. 21.6). Other injuries included in this group include small subcapsular (Fig. 21.7) or perinephric hematomas, small cortical lacerations (Fig. 21.8), subsegmental renal infarcts, and rarely pyelosinus extravasation associated with blunt injury. In general, these injuries do not involve a break in the renal capsule.
TABLE 21.1 Renal Injury Scale of the American Association of Surgeons in Trauma
Grade
Injury Description
1
Microscopic or gross hematuria with normal findings of imaging studies; renal contusion; nonexpanding subcapsular hematoma without parenchymal laceration
2
Nonexpanding perirenal hematoma confined to the retroperitoneum; superficial lacerations (<1 cm depth) in the renal cortex
3
Lacerations >1 cm depth in the renal cortex without extension into the collecting system or urinary extravasation
4
Lacerations extending through the renal cortex, medulla, and collecting system; injuries to the main renal artery or vein with contained hemorrhage; thrombosis of a segmental renal artery without parenchymal laceration
5
Lacerations that completely shatter the kidney; injuries to the renal hilum with devascularization of the kidney; traumatic renal arterial occlusion
Traumatic pyelosinus extravasation may occur from minor injuries or may be demonstrated in patients with preexisting renal calculi that become lodged in the UPJ after injury. It may also occur in patients with congenital renal anomalies, such as horseshoe kidney or UPJ obstruction. In patients with no detectable underlying abnormality, it is assumed to be caused by transient obstruction of the ureter, possibly by a blood clot.
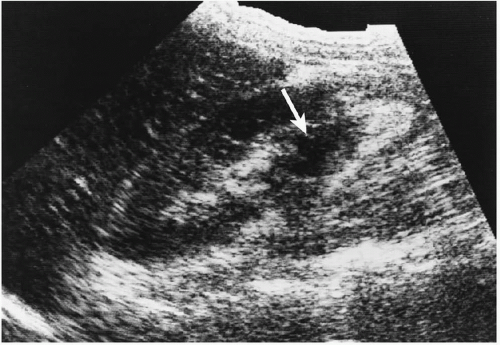
On US, intrarenal hematomas are seen as poorly marginated areas of decreased echogenicity within the cortex (Fig. 21.9).
On CT, intrarenal hematomas (Figs. 21.6) are seen as rounded or ovoid, poorly marginated areas of decreased attenuation within the renal parenchyma; in some cases, the small intrarenal lacerations with which they are associated may be visualized extending into the hematoma itself (Fig. 21.8). Subcapsular hematomas appear as rounded or elliptical areas of decreased attenuation located between the renal cortex and the renal capsule (Fig. 21.10). Such hematomas indent or flatten the renal margins as they exert a compressive force against the kidney. Perinephric hematomas are located between the renal capsule and Gerota facia. They do not indent or flatten the renal contour (Fig. 21.11) and are usually associated with an intrarenal hematoma (Fig. 21.12). Perinephric hematomas may be quite large and may extend inferiorly into the true pelvis following the cone of renal fascia, may displace the kidney anteriorly, or occasionally may be quite localized and simulate a subcapsular collection.
TABLE 21.2 Radiologic Classification of Blunt Renal Injuries
Category
Disease Extent
I
Small intrarenal (contusions) or subcapsular hematomas, lacerations, subsegmental cortical infarcts
II
Deep cortical lacerations with or without involvement of the collecting system; segmental infarcts
III
Catastrophic renal injuries including multiple lacerations, shattered kidney, or vascular injuries involving the renal pedicle
IV
Avulsion of the UPJ
FIGURE 21.6. Intrarenal hematoma. CT shows subtle low attenuation foci in the left kidney representing intrarenal hematoma.
FIGURE 21.7. A small subcapsular hematoma is present on the posterior aspect of the right kidney.
The attenuation coefficient of these hematomas depends on their age, with acute hematomas having a higher attenuation value than unenhanced renal parenchyma (Fig. 21.13). With time, their attenuation value decreases because of liquefaction of the clot. In addition, the measured attenuation value of these perinephric hematomas may be lower than expected, reflecting their tendency to infiltrate the normal perinephric fat.
Intermediate Injuries
Intermediate injuries constitute approximately 10% of the cases of renal injury. They are usually managed conservatively, but may, on occasion, require surgical intervention, particularly if clinical deterioration develops. Injuries in this category include major renal lacerations that extend beyond the renal capsule, with or without involvement of the renal collecting system. These lacerations, which when distracted are termed fractures, may be sufficiently large to be visible radiographically. Extensive perirenal hematomas are usually present and, if the laceration involves the collecting system, demonstrate extravasation of contrast medium on radiologic examination. Vascular injuries involving the segmental renal vessels are usually included in this category.
The diagnosis of major lacerations (Fig. 21.14) can be made on CT when a hematoma-filled cleft that extends through the renal capsule is visualized in the renal parenchyma. If the laceration extends into the renal collecting system, opacified urine will extravasate into the lateral perinephric space (Fig. 21.15). If the lacerated segment has become devitalized, this portion of the kidney will not enhance after contrast administration. Because this segment is surrounded by hematoma and does not enhance, it may be difficult to appreciate as a separate fragment.
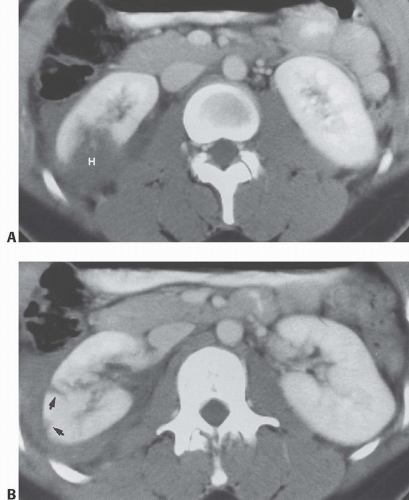
FIGURE 21.8. Renal laceration with intrarenal hematoma. A: CT scan through the right kidney shows an intrarenal hematoma (H). B: More caudal section shows two small lacerations (arrows) and a small perinephric hematoma.
FIGURE 21.9. Intrarenal hematoma. Longitudinal US shows decreased echogenicity in the area of the hematoma (arrow) and slight anterior displacement of the lower pole of the right kidney.
Traumatic arteriovenous fistulae almost always result from penetrating or iatrogenic renal injury. The vast majority occur after percutaneous renal biopsy, are not hemodynamically significant, and close spontaneously. Clinically, symptomatic lesions may present with hypertension, evidence of left heart failure, or an audible bruit on physical examination. On angiography, opacification of a large draining vein is visible during the arterial phase of the study. The draining vein is usually saccular in appearance; with hemodynamically significant lesions, there may be decreased nephrographic staining and evidence of renal ischemia.
FIGURE 21.10. Subcapsular hematoma. The hematoma is contained within the renal capsule compressing the renal parenchyma.
FIGURE 21.11. Perinephric hematoma. The hemorrhage extends into the perinephric space and does not compress the renal parenchyma.
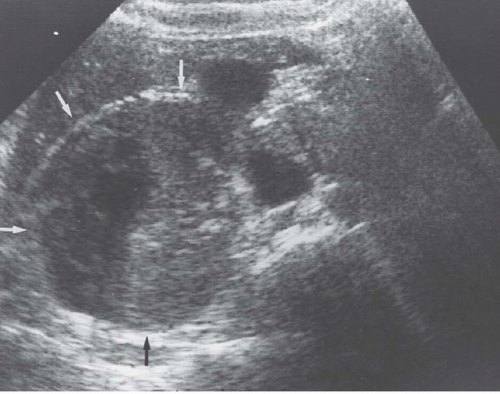
FIGURE 21.12. Perinephric hematoma. Transverse sonogram shows the large perinephric collection (arrows).
FIGURE 21.13. Large subcapsular hematoma. A: Precontrast scan shows high-density blood adjacent to the left kidney, indicating acute hemorrhage. B: On the postcontrast study, a relatively thick rind is seen surrounding the hematoma.
FIGURE 21.14. Renal laceration. A large renal laceration is present in the left kidney associated with a moderate perinephric hematoma.
FIGURE 21.15. Renal laceration with extension into the collecting system. A, B: Postcontrast CT shows a distracted renal laceration (fracture) that extends into the collecting system with contrast extravasation into the perinephric space.
Traumatic arterial pseudoaneurysms are rare injuries that almost always occur after penetrating trauma. Although the diagnosis may be suspected by CT, definitive diagnosis requires angiography (Fig. 21.16).
Occlusion of a segmental renal vessel is the most common vascular injury of the kidney after blunt renal trauma. Such occlusion results in segmental renal infarction. On CT, infarcts appear as sharply demarcated wedge-shaped areas of diminished or absent contrast enhancement that extend to the renal cortex (Fig. 21.17). If the capsular blood supply remains intact, perfusion of the outer layer of cells results in enhancement of the cortical rim (Fig. 21.18). Most commonly, segmental or cortical infarcts are not associated with a perinephric hematoma, thereby helping to distinguish them from intrarenal hematomas. The sensitivity of CT for the detection of such injuries can be enhanced with the use of early-phase scanning. Indeed, the ability of CT to reliably distinguish these injuries from hematomas depends on the contrast enhancement provided by the bolus of contrast medium. If there has been too long an interval between the contrast administration and the CT study, their sharply marginated appearance will be lost because of collateral circulation.
FIGURE 21.16. Posttraumatic pseudoaneurysm. A: A selective right renal arteriogram demonstrates a traumatic pseudoaneurysm in the lower pole of the kidney in a patient who suffered a stab wound. B: Following embolization, the pseudoaneurysm is no longer present. A subsegmental renal infarct is also present in the upper pole.
Segmental renal infarcts are demonstrated on angiography as wedge-shaped areas of absent vascular perfusion. The occluded artery responsible for the infarct can usually be identified by its sharply cutoff appearance (Fig. 21.19). Collateral vascular supply through capsular branch vessels may also be identified angiographically.
▪ POSTTRAUMATIC CONTRAST EXTRAVASATION
Common
Renal parenchymal laceration extending into the collecting system
Uncommon
Posttraumatic pyelosinus extravasation
UPJ laceration or avulsion
FIGURE 21.17. A: Large segmental infarct. CT shows a large area of absent contrast enhancement corresponding to the posterior segmental branch of the right renal artery. B: Follow-up CT 2 years later shows scarring in the distribution of the infarct.
Major Injuries
Major injuries, which account for approximately 5% of all renal injuries, virtually always require surgical exploration or radiologic intervention, because of a threat to the viability of the kidney or because of life-threatening hemorrhage. In such situations, immediate transcatheter embolization is often performed, although surgical exploration and nephrectomy may be necessary. Major renal injuries include multiple renal lacerations or injury of the renal pedicle including avulsion or laceration of one or more of the renal veins (Fig. 21.20), and thrombosis or laceration of the main renal artery. With multiple lacerations, large perinephric hematomas are common, and the tamponade effect of the renal fascia may be lost if it is also torn. Multiple devitalized segments of renal parenchyma may be present (Fig. 21.21), and active extravasation of contrast material indicative of active bleeding may be seen.
Traumatic Renal Infarction
Traumatic renal artery thrombosis is reported to occur in approximately 3% of patients suffering renal injuries. The injury occurs as a result of a contrecoup tearing of the intima of the renal artery in patients suffering acute deceleration. The resulting intimal flap causes thrombosis of the renal artery. The injury generally occurs in patients suffering a fall from a height or as a result of an autopedestrian accident. Although gross or microscopic hematuria is often present, it may be absent in as many as 25% of patients.
FIGURE 21.18. Segmental renal infarct. There is no enhancement of the lateral portion of the left kidney. The outer layer of cells is preserved because the cells’ arterial supply comes from capsular vessels.
The majority of patients suffering global renal infarction eventually develop irreversible loss of renal function and parenchymal atrophy. There are, however, isolated reports of spontaneous recovery of some renal function. In such cases, it is presumed that collateral renal circulation has preserved a small amount of functioning parenchyma.
Thrombosis of the main renal artery results in complete absence of contrast enhancement on CT when studied shortly after injury (Fig. 21.22). In some cases, and especially those in whom the diagnosis of pedicle injury is delayed, a rim of enhancement in the outer renal cortex may be present (cortical rim sign) because of circulation from capsular and collateral vessels (Fig. 21.18). There may also be enhancement of the wall of the renal pelvis because of collateral flow through periureteric vessels. Similar findings are frequently present in patients with nontraumatic renal infarction. In the majority of patients with this injury, there will be no evidence of a perinephric or subcapsular hematoma, unless this injury has been caused by a penetrating wound or is associated with injury of another organ. Retrograde opacification of the renal vein of the affected kidney has been reported as a secondary sign of this injury.
Only gold members can continue reading. Log In or Register to continue